HYPOCALCEMIA HOANG CUONG MD HMU Blogger Hoangcuonghmu wordpress

HYPOCALCEMIA HOANG CUONG MD, HMU Blogger: Hoangcuonghmu. wordpress. com

Definition • Normal Serum Calcium: 8. 5 -10. 5 mg/d. L. • Hypocalcemia: a total serum calcium level <8. 5 mg/d. L or an ionized calcium level <2. 0 mg/d. L.

Background - Involved in: cell death, duration and strength of cardiac muscle contraction, muscle contraction in blood vessels, airways and uterus, coagulation, bone metabolism, neurotransmitter and hormone. . - Exists in two states: • Free ionized form (approx. . 50%) • Bound to other molecules (primarily albumin) - Ionized Ca 2+ concentration is inversely proportional to p. H → An ↑ p. H results in a ↓ in ionized Ca 2+ - Ca 2+ metabolism: • Vitamin D: Aids in intestinal Ca 2+ absorption
 § Increased renal Ca 2+ reabsorption § Arbitrates Vit D")
Background • Parathyroid hormone(PTH) § Increased renal Ca 2+ reabsorption § Arbitrates Vit D stimulated intestinal Ca 2+ absorption. § Mobilizes Ca 2+ form bone • Carcitonin: § PTH antagonist § Inhibits renal Ca 2+ reabsorption § Inhibits Ca 2+ mobilization from bone Ø Ca 2+ plays numerous critical roles including muscle contraction (skeletal and smooth), clotting factor activity and nerve conduction

Causes - Intake reduced: • Ca 2+ • Vitamin D • Phenytoin (increased metabolism of vitamin D) • • Redistribution: Alkalosis Citrate toxicity Electrolyte disorders: Hypomagnesemia, hyperphosphatemia Severe pancreatitis.

Causes • Abnormal cell destruction: tumor lysis syndrome, rhabdomyolysis. • Hypoparathyroidism • Decreased bone turnover • Drugs: Biphosphonates, PPI’s, SSRI’s, gentamycin… - Output increased: • Urinary: Ethylene glycol, cis-plastin, protamine, loop diuretics. • Non-urinary: Bleeding, plasmapheresis, citrated RRT.

Causes Ø Causes of hypocalcemia and acid-base disturbance: • Metabolic alkalosis: Citrate toxicity, hyperventilate • Metabolic acidosis: acute renal failure, tumor lysis, rhabdomyolysis, pancreatitis, ethylene glycol poisoning, hydrofluoric acid, sepsis, burns.
 Magnesium")
Causes of Ionized Hypocalcemia in the ICU: Alkalosis Fat Embolism Blood Transfusions (15%) Magnesium Depletion (70%) Brugs: • Aminoglycosides • Heparin (10%) Pancreatitis Renal insufficiency (50%) Sepsis (30%)

Causes
 • Low albumin hypocalcemia:")
- Conditions →Changes in total calcium (without affecting ionized calcium) • Low albumin hypocalcemia: - Conditions →Changes in ionized calcium (without affecting total calcium) • Alkalemia→ ↑ ionized calcium binding to albumin→ ↓ Ionized calcium levels. • Hyperphosphatemia→ ↓ ionized calcium binding to albumin→ ↓ Ionized calcium levels.

Neuromuscular Acute Paresthesia, Tetany, Carpopedal spasm Trousseau’s sign, Chvostek’s sign Seizure Laryngospasm Cardiac Clinical Manifestations QT prolongation Hypotension Heart failure Arrhythmia

Clinical Manifestations Central Nervous System Chronic Basal ganglia calcifications EPS Parkinsonism Dementia Ophthalmologic Cataracts
 Seizures")
→ History: - Perioral numbness Paresthesias Muscle cramps Mild mental status changes (irritability) Seizures Tetany Collapse To find cause: Diet, drug, symptoms specific to cause. Laryngospasm

→ Examination: Trousseau's sign: • Carpal spasms induced by inflation of a blood pressure cuff 20 mm Hg above systolic BP for 3 minutes. • Adduction of the thumb, Flexion of the MCP joints. Extension of the IPJ. Flexion of the wrist → Neuromuscular irritability. (commonly seen in patients without hypocalcemia)
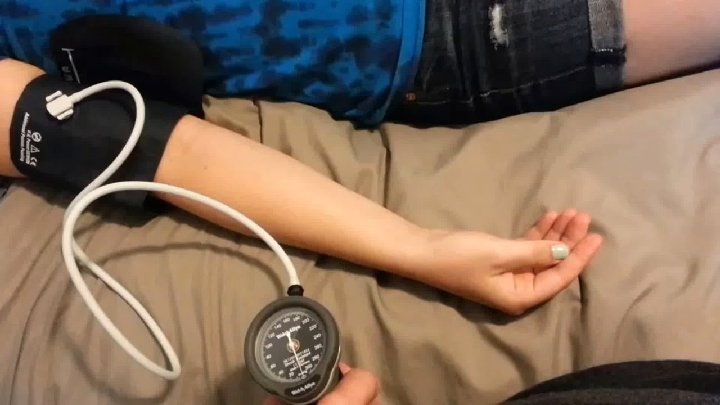

→ Examination: Trousseau’s sign: Chvostek’s sign is the twitching of the facial muscles in response to tapping over the area of the facial nerve.

→ Examination: • • How to measure QT interval? QTc prolongation primarily by prolonging the ST segment. The T wave is typically left unchanged. Dysrhythmias are uncommon. Torsades de pointes may occurs.
 PO 43 - , Mg 2+")
Investigations - ECG Ca 2+ (total and ionized) PO 43 - , Mg 2+ PTH Amylase, Lipase (rule out pancreatitis) U+E →Renal failure, hyperkalaemia CK and urate →Rhabdomyolysis

Managements - Asystomatic/Minimally symptomatic: Ø Oral supplementation with Calcium salt. - Moderate/Severe symptoms: Ø Intravenous calcium supplementation: 100 -300 mg Ca 2+ → ↑ Ca 2+ by: 0. 5 -1. 5 m. Eq Ø Calcium Chloride (Ca. Cl 2): 10 ml of Ca. Cl 2=270 mg of Ca 2+ Ø Calcium Gluconate: 10 ml of 10% Ca. Gluconate= 90 mg of Ca 2+ - Magnesium supplementation: → Concomitant hypomagnesimia is common.
![IV: intravenous. * Corrected calcium [Ca] = Measured total [Ca] + (0. 8 ×](http://slidetodoc.com/presentation_image_h/1b58e970b4732ee95e46ce56303d986b/image-20.jpg "IV: intravenous. * Corrected calcium [Ca] = Measured total [Ca] + (0. 8 ×")
IV: intravenous. * Corrected calcium [Ca] = Measured total [Ca] + (0. 8 × (4. 0 – [albumin]))
- Slides: 20