UNIT II COMMON SIGNS SYMPTOMS TOPIC Electrolyte imbalanceshyponatremia

UNIT –II COMMON SIGNS & SYMPTOMS TOPIC: Electrolyte imbalanceshyponatremia and hypernatremia Prepared by, Mrs. Anju Ullas Lecturer Dept. of Medical Surgical Nursing Yenepoya Nursing College

Introduction Electrolyte imbalance is an abnormality in the concentration of electrolytes in body. Electrolytes play a vital the role in maintaining homeostasis within the body. They help to regulate heart and neurological function, fluid balance, oxygen delivery, acid–base balance and much more.

Electrolytes • Na+: most abundant electrolyte in the body. • K+: essential for normal membrane excitability for nerve impulse. • Cl-: regulates osmotic pressure and assists in regulating acid-base balance.

• Ca 2+: usually combined with phosphorus to form the mineral salts of bones and teeth, promotes nerve impulse and muscle contraction/relaxation • Mg 2+: plays role in carbohydrate and protein metabolism, storage and use of intracellular energy and neural transmission. Important in the functioning of the heart, nerves, and muscles

Normal electrolyte values • Sodium: 135 -145 m. Eq/L • Potassium: 3. 5 -5 m. Eq/L • Calcium: 8. 5 – 10. 2 mg/ d. L • Chloride: 98 -107 m. Eq/L • Magnesium: 1. 5 -2. 5 m. Eq/L
 • Hypernatremia (sodium")
Major electrolyte imbalances • Hyponatremia (sodium deficit < 130 m. Eq/L) • Hypernatremia (sodium excess >145 m. Eq/L) • Hypokalemia (potassium deficit <3. 5 m. Eq/L) • Hyperkalemia (potassium excess >5. 1 m. Eq/L) • Hypocalcemia (calcium deficit <8. 5 mg/d. L) • Hypercalcemia (calcium excess <10. 2 mg/d. L) • Chloride imbalance (<98 m. Eq/L or >107 m. Eq/L) • Magnesium imbalance (<1. 5 m. Eq/L or >2. 5 m. Eq/L)

Sodium • Hyponatremia • Hypernatremia

Hyponatremia
 are subject to more")
• Acute hyponatremia (developing over 48 hr or less) are subject to more severe degrees of cerebral edema • Chronic hyponatremia (developing over more than 48 hr) experience milder degrees of cerebral edema

Types of hyponatremia • Hypovolemic hyponatremia • Euvolemic hyponatremia • Hypervolemic hyponatremia • Redistributive hyponatremia

• Hypovolemic hyponatremia Develops as sodium and free water are lost and/or replaced by inappropriately hypotonic fluids Sodium can be lost through renal or non-renal routes

Nonrenal loss: v GI losses Vomiting, Diarrhea, fistulas, pancreatitis v Excessive sweating v Third spacing of fluids ascites, peritonitis, pancreatitis, and burns v Cerebral salt-wasting syndrome traumatic brain injury, aneurysmal subarachnoid hemorrhage, and intracranial surgery

Renal Loss: v Acute or chronic renal insufficiency v Diuretics

Euvolemic hyponatremia Sodium deficit is more and the water volume remains same. Etiology: Psychogenic polydypsia, often in psychiatric patients Administration of hypotonic intravenous (5% Dextrose) o r irrigation fluids ( sorbitol, glycerin) in the immediate postoperative period

administration of hypotonic maintenance intravenous fluids Infants who may have been given inappropriate amounts of free water bowel preparation before colonoscopy or colorectal surgery

Hypervolemic hyponatremia Total body sodium increases, and total body water increases to a greater extent. Can be renal or non-renal acute or chronic renal failure vdysfunctional kidneys are unable to excrete the ingested sodium load cirrhosis, congestive heart failure, or nephrotic syndrome

Redistributive hyponatremia Water shifts from the intracellular to the extra cellular compartment, with a resultant dilution of sodium. The total body water and total body sodium are unchanged. This condition occurs with hyperglycemia Administration of mannitol

Signs and symptoms • Nausea and vomiting • Headache • Confusion • Loss of energy, drowsiness and fatigue • Restlessness and irritability • Muscle weakness, spasms or cramps • Seizures • Coma

Diagnostic evaluation • Blood tests. • Urine tests.

Complication • In acute hyponatremia, sodium levels drop rapidly — resulting in potentially dangerous effects, such as rapid brain swelling, which can result in a coma and death.

Medical management • Determine cause of hyponatremia and to correct it. • If client has hyponatremia due to fluid volume excess, intake of fluids will be restricted to allow the sodium to regain balance. • If the serum sodium level falls below 125 m. Eq/L, sodium replacement is needed.

Pharmacologic management • For client with moderate hyponatremia 125 meq/ L - IVsolution (0. 9% Na. Cl) or lactated Ringer solution may be ordered. • When the serum sodium level is 115 meq / L or less, a concentrated saline solution such as 3 % Na. Cl is indicated.

Nursing management Assessment • Monitor cardiovascular, neuromuscular, cerebral, respiratory, renal, and gastrointestinal status of the client. Monitor vital signs as well as central venous pressure, if available. Weigh client daily. Observe for sudden weight gain or loss

• Note presence of neck and peripheral vein distention, along with pitting edema, and dyspnea. • Auscultate lung and heart sounds. • Monitor intake and output. • Monitor infusion rate of parenteral fluids closely

Nursing diagnosis Fluid volume excess May be related to • Excess fluid or sodium intake. • Compromised regulatory mechanism. • Possibly evidenced by • Ascites. • Aphasia, muscle twitching, tremors, seizures. • Bounding pulses. • Changes in the level of consciousness (lethargy, disorientation, confusion to coma). • Crackles.

Fluid volume deficit May be related to • Active fluid loss-burns, diarrhea, fistulas, gastric intubation, hemorrhage, wounds. • Regulatory failure- diabetes insipidus, diabetic ketoacidosis (DKA), adrenal disease, systemic infections, recovery phase of acute renal failure. • Possibly evidenced by • Abdominal distention. • Confusion, restlessness.

Nursing diagnosis Risk For Electrolyte Imbalance May be related to o Diarrhea, vomiting. o Renal dysfunction. o Treatment-related side effect such as medications, gastric suctioning, electrolyte-free intravenous (IV) solutions. o Water intoxication.

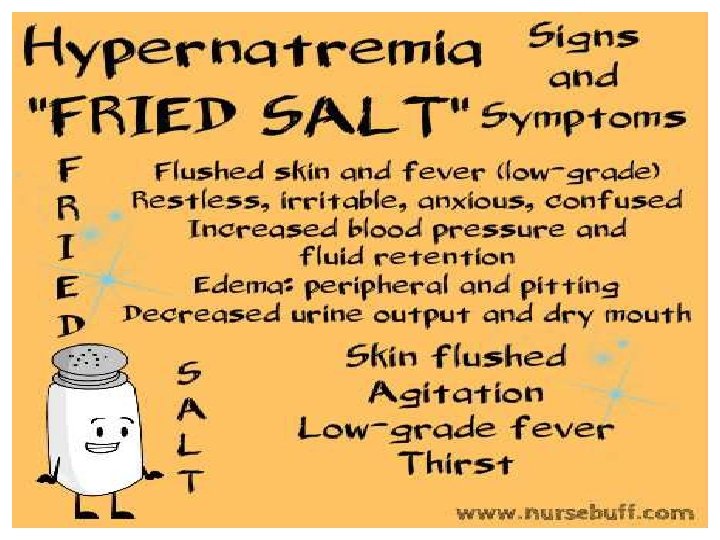
Hypernatremia is an electrolyte imbalance and is indicated by a high level of sodium in the blood. The normal adult value for Na is 135 -145 m. Eq/L. It implies a deficit of total body water relative to total body Na, caused by water intake being less than water losses.

Causes of hypernatremia • Excess water loss : eg- heat exposure, diabetes insipidus, vomiting diarrhea, • Impaired thirst: eg - primary hypodypsia • Excessive Na+ retention • Excessive salt intake • Hyperventilation • Obstructive uropathy • Heavy exercise, exertion

• Drugs such as steroids and certain blood pressure lowering medicines. • Dehydration from not drinking enough water • Administration of hypertonic enteral feedings with out adequate water supplements.

Clinical manifestations • Increased thirst • Restlessness and agitation • Weight loss and generalized weakness • Disorientation, delusions and hallucinations • Decreased level of consciousness • Anorexia, nausea and vomiting • Flushed skin, peripheral and pulmonary edema

• • Pitting edema Abnormal skin turgor Postural hypertension Dyspnea and respiratory arrest.

Diagnostic evaluation • Blood tests. • Urine tests.

Management Goals • • Recognition of the symptoms, when present Identification of the underlying causes Correction of volume disturbances Correction of hypertonicity

• correct water deficit • Rate of correction : v. Acute hypernatremia- 1 m. Eq/L/hr v. Chronic hypernatremia-1 m. Eq/L/hr or 10 m. Eq/L over 24 hr Rapid correction may lead to cerebral edema

Dietary management

Complications • • • Cerebral bleeding. Cerebral edema Subarachnoid hemorrhage Permanent brain damage Death due to brain shrinkage

Nursing management Assessment • Check the patient’s vital signs; fever, tachycardia, decreased blood pressure, and orthostatic hypotension are characteristic of hypernatremia and compare with prior. • Check the skin and mucous membranes for signs of dehydration (poor skin turgor; flushed skin color; dry mucous membranes and a rough, dry tongue).

• Assess the patient for muscle twitching, hyperreflexia, tremors, seizures, and rigid paralysis. • Check the patient’s ability to obtain adequate fluid intake as lethargic state contributes to the poor fluid intake. • Assess the safety measures for the patient, especially for the disoriented elderly or debilitated patient.

• Check the patient’s level of consciousness and her or his ability communicate needs. • Checks weight everyday to monitor the fluid volume status. • Assess I/O chart.

Fluid volume deficit May be related to • Active fluid loss-burns, diarrhea, fistulas, gastric intubation, hemorrhage, wounds. • diabetes insipidus, diabetic ketoacidosis (DKA) • Possibly evidenced by • Abdominal distention. • Confusion, restlessness.

Risk For Electrolyte Imbalance May be related to o Diarrhea, vomiting. o Treatment-related side effect Possibly evidenced by • Confusion, restlessness.

Meaning Hypokalemia is a serum potassium level less than 3. 5 m. Eq /L

Etiology • decreased potassium intake • increased losses or shifts in intracellular and extracellular distribution.
 v. Gastrointestinal • Prolonged diarrhoea •")
Increased losses (split to renal and gastro losses) v. Gastrointestinal • Prolonged diarrhoea • Vomiting • Excessive use of laxatives

v. Renal • Diuretic therapy* • Urinary loss in congestive heart failure • Hypomagnesaemia • Primary or secondary hyperaldosteronism • Cushings syndrome or disease • Large doses of corticosteroids

Pathophysiology Causes Decreased sodium and bicarbonate serum level Decreased perfusion pressure in the renal arterioles Juxtaglomelular cells release Converted Angiotensin I from Angiotensin

Pathophysiology Converted Angiotensin II from Angiotensin I Release of Constricts the arterioles the aldosterone Acts on renal tubular and gastrointestinal epithellium Increased activity of the proximal tubule Na+/H+

Pathophysiology Elevated distal Increased H+ excretion tubule flow rate and bicarbonate Increased tubular lumen electronegativity Increased sodium reabsorbed from tubular urine back to the bloodstream Potassium moves from the bloodstream into the tubule

Pathophysiology Increased renal excretion of potassium HYPOKALEMIA Signs and symptoms

Signs and symptoms

Signs and symptoms

Laboratory and Diagnostic Findings • Serum potassium levels less than 3. 5 m. Eq/L • ECG changes- flat/inverted T waves, depressed ST segment, elevated U wave • Metabolic alkalosis • Urinary potassium excretion test exceeding 20 m. Eq/day

Complications Heart problems Paralysis

Management Medical management • Determining & correcting the cause of the imbalance. • Extreme hypokalemia requires cardiac monitoring

Management Pharmacological management Oral potassium replacement therapy is usually prescribed for mild hypokalemia. Potassium is extremely irritating to gastric mucosa; therefore the drug must be taken with Glass of water or juice or during meals. Potassium chloride can be administered intravenously for moderate or severe hypokalemia & must be diluted in IV fluids.

Management Pharmacological management • Administration of potassium by IV push may result in cardiac arrests. Potassium can be given in doses of 10 to 20 m. Eq/ hour diluted in IV fluid if the client is on heart monitor. • High concentration of potassium is irritating to heart muscle. Thus correcting a potassium deficit may take several days.

Management Nutritional management The administration of foods that are high in potassium help to correct the problem as well as prevent further potassium losses.

Management Nursing management Assessment • History collection • Physical examination • Identify ECG changes such as depressed T waves, peaking P waves. • Observe for dehydration. Accurately record state of hydration. • Observe for neuromuscular changes such as fatigue and muscular weakness.

Management Nursing management Assessment • Record fluid intake and output. • Check blood volume and venous pressure.

Management Nursing diagnosis Fluid volume deficit May be related to • Active fluid loss-burns, diarrhea, fistulas, gastric intubation, hemorrhage, wounds. • diabetes insipidus, diabetic ketoacidosis (DKA) • Possibly evidenced by • Abdominal distention. • Confusion, restlessness.

Management Nursing diagnosis Risk For Electrolyte Imbalance May be related to o Diarrhea, vomiting. o Renal dysfunction. o Treatment-related side effect such as medications, gastric suctioning, electrolyte-free intravenous (IV) solutions. o Water intoxication.

Management Nursing diagnosis Risk for injury related to muscle weakness Risk for ineffective health maintenance related to lack of knowledge about how diuretic therapy and laxative affect potassium levels

Hyperkalemia is an Elevated potassium level over 5. 0 m. Eq/L.

Hyperkalemia ETIOLOGY • Retention of Potassium- Renal insufficiency, renal failure, • decreased urine output, potassium sparing diuretics. • Excessive release of Cellular Potassium - severe traumatic injuries. Severe burns, severe infection, metabolic acidosis. • Excessive IV infusions or Oral administration of potassium.

Hyperkalemia

Hyperkalemia

Lab findings

Medical management • When serum potassium level is 5. 0 to 5. 5 m. Eq/L restrict potassium intake. • If potassium Excess is due to metabolic acidosis, correcting the acidosis with sodium bicarbonate promotes potassium uptake into the cells. • Diuretics- Improving urine output decreases elevated serum potassium level.

Nutrition management

Nursing management Assessment v History collection v Physical examination v Assessment of cardiovascular, respiratory, neuromuscular, renal, and gastrointestinal status; place the client on a cardiac monitor.

Nursing diagnosis • Activity intolerance related to skeletal muscle weakness as evidenced by • Excess fluid volume related to renal failure as evidenced by • Risk for decreased cardiac output related to hyperkalemia as evidenced by • Risk for ineffective health maintenance related to inadequate knowledge of recommended diet as

References 1. Black MJ. Textbook of medical surgical nursing. 7 th ed. St. louis: Saunders 2. Brunner. Text book of medical surgical nursing. 6 th ed. Philadelphia: Saunders 3. Lewis. Medical surgical nursing. 6 th ed. St louis: Mosby
- Slides: 77