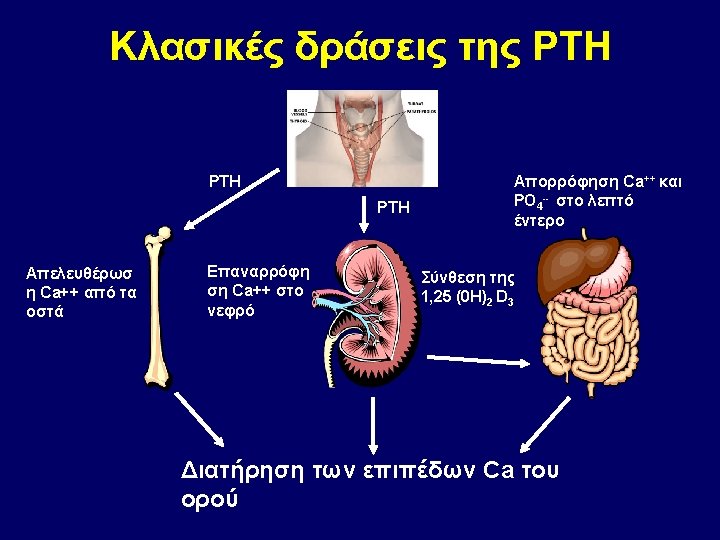
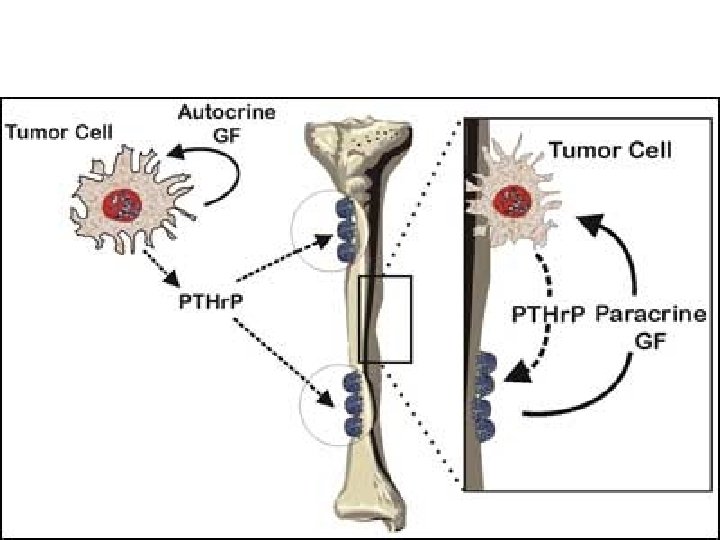
PTHr P PTH Schematic illustration of impact of




 calcium-PTH dynamics in normal subjects and patients receiving lithium carbonate")

 25: 2347– 2357")



 • Based on 5490 individuals • Use of t.")
 •")
 Osteoporosis Vitamin D")


Vit D ΑΦ Ρ Ca Ca Ούρων 24 h PTH Conclusion Vitamin D replacement")
 BMD increased in LS by 2.")


")







")
![Κλασματική απέκρισση Ca Ca/Cr clearance ratio = [24 -hour Urine Ca x serum Cr]](https://slidetodoc.com/presentation_image_h/1a9d3865a17e81b848c87c729f0a05b5/image-72.jpg "Κλασματική απέκρισση Ca Ca/Cr clearance ratio = [24 -hour Urine Ca x serum Cr]")















 assays in patients with hypercalcemia of malignancy")
- Slides: 105
PTHr. P / PTH
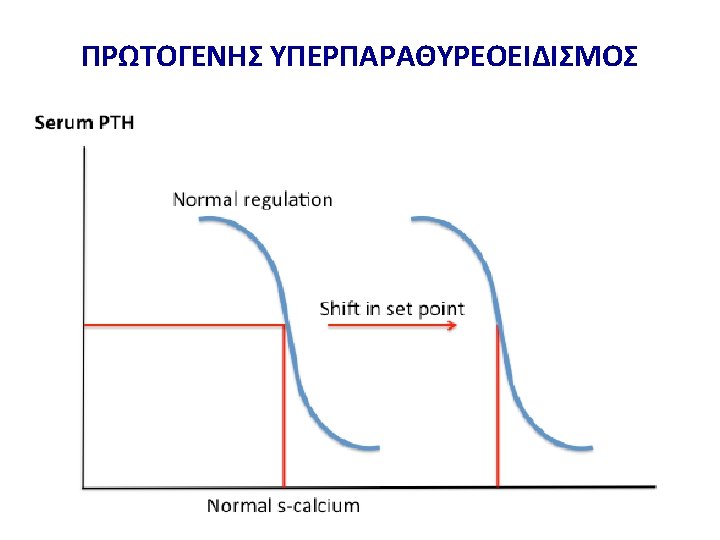
Schematic illustration of impact of changes in Ca 2+ - sensitivity on set-point
Mean (±SD) calcium-PTH dynamics in normal subjects and patients receiving lithium carbonate
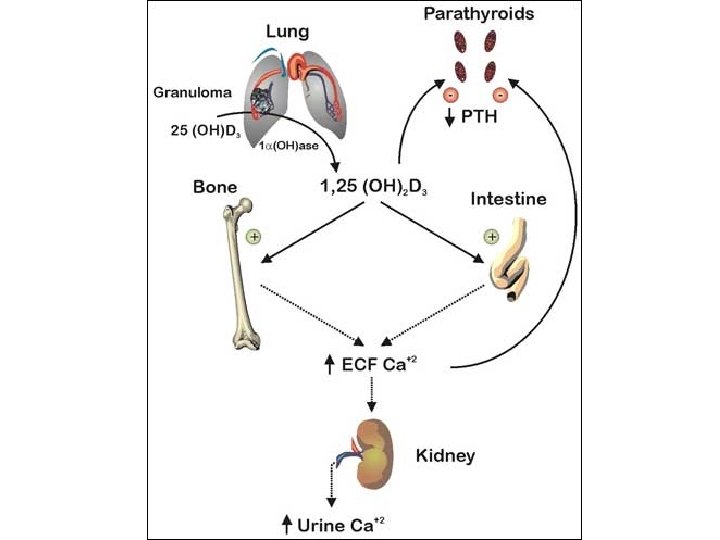
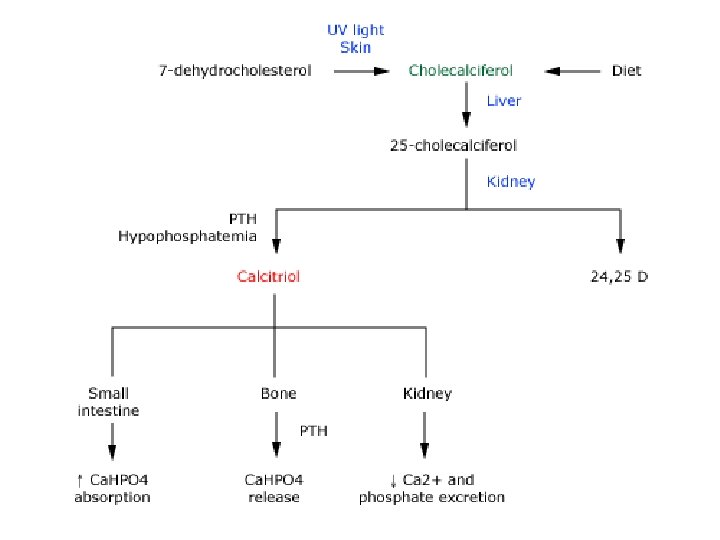
Pathways of vitamin D synthesis
Osteoporos Int (2014) 25: 2347– 2357
Changes in systemic calcium metabolism during pregnancy Best Practice & Research Clinical Endocrinology & Metabolism 25 (2011) 975– 983
Changes in systemic calcium metabolism during lactation Best Practice & Research Clinical Endocrinology & Metabolism 25 (2011) 975– 983
Schematic illustration contrasting calcium homeostasis in human pregnancy and lactation compared with normal Pregnancy-induced changes in maternal Ca metabolism Intestinal Ca absorption↑ Urinary Ca excretion↑ “Absorptive hypercalciuria” Total Ca ↓ Ca++ ↔ PTH ↓ PTHr. P ↑ E 2, PRL, Placental Lactogen ↑ Bone resorption markers ↑ BMD ↔↓ Fetal Ca metabolism Ca: 25 -30 g Ca higher than the mother PTH↓ Calcitonin ↑
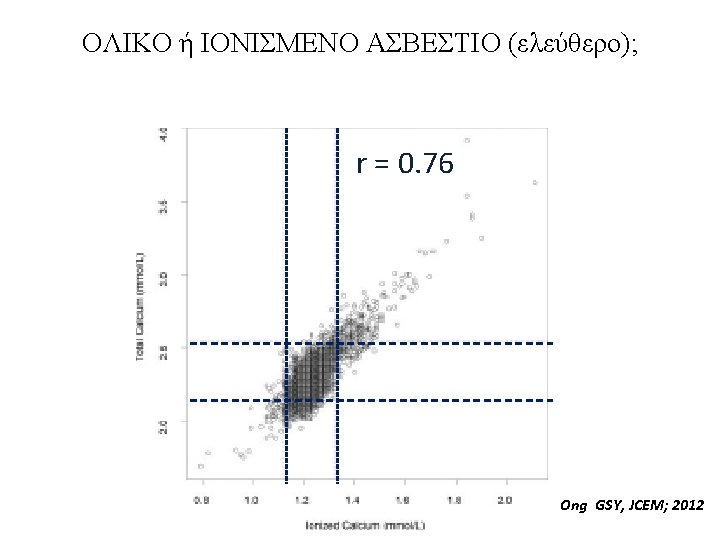
ΟΛΙΚΟ ή ΙΟΝΙΣΜΕΝΟ ΑΣΒΕΣΤΙΟ (ελεύθερο) • Based on 5490 individuals • Use of t. Ca alone would miss 45% of i. Ca based hypercalcemic pas • In verified PHPT, 10% of pas with normal t. Ca had elevated i. Ca Ong GSY, JCEM; 2012
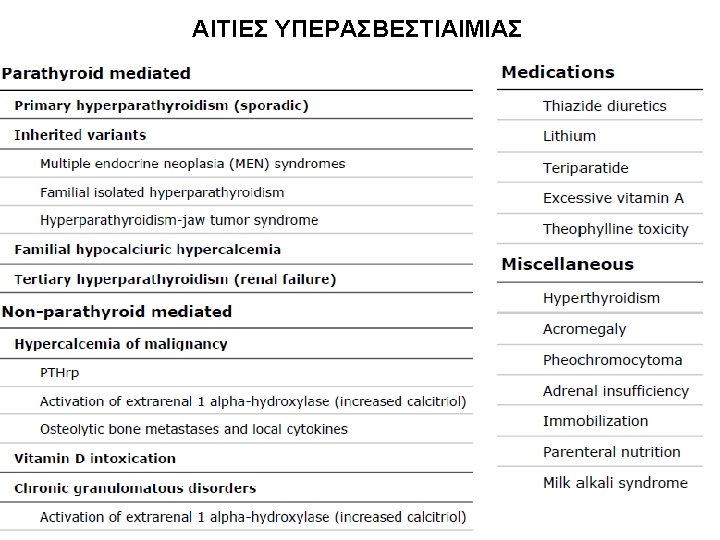
Hypocalciuria • Incomplete collection • Drugs (thiazide diuretics, benzothiadiazide diuretics chlorthalidone, and estrogen) • Hypoparathyroidism • Pseudohypoparathyroidism (a lack of response to PTH rather than decreased secretion of PTH), rickets • Hypothyroidism • Steatorrhea • Nephrosis • Familial Hypocalciuric Hypercalcemia (FHH)
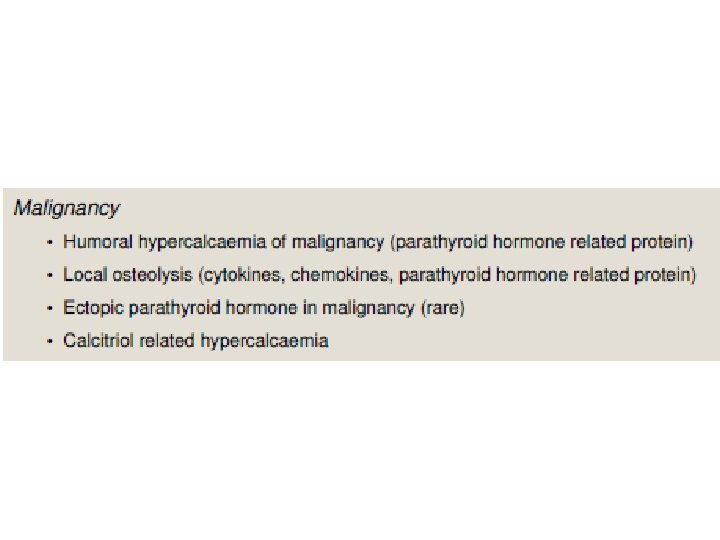
Hypercalciuria • • • Hyperparathyroidism Multiple myeloma (or any osteolytic neoplasm) Osteoporosis Vitamin D overdose Renal tubular acidosis Hyperthyroidism Paget's disease Sarcoidosis Drugs (Antacids, Calcium supplements, Spironolactone, Androgens, Growth Hormone, Acetazolamide and Corticosteroids)
Causes and mechanisms of hypercalcemia Curr Opin Nephrol Hypertens 2013, 22: 371– 376
Clinical manifestations of hypercalcemia Renal Musculoskeletal • • • Polyuria Polydipsia Nephrolithiasis Nephrocalcinosis Distal renal tubular acidosis Nephrogenic diabetes insipidus • Acute and chronic renal insufficiency • • • Gastrointestinal Cardiovascular • Nausea, vomiting • Bowel hypomotility and constipation • Pancreatitis • Peptic ulcer disease Muscle weakness Bone pain Osteopenia/osteoporosis Neurologic • • Decreased concentration Confusion Fatigue Stupor, coma Shortening of the QT interval Bradycardia Hypertension
25(ΟΗ)Vit D ΑΦ Ρ Ca Ca Ούρων 24 h PTH Conclusion Vitamin D replacement in subjects with PHPT and coexistent vitamin D deficiency increase 25 (OH) D and reduce serum PTH significantly without causing hypercalcaemia and hypercalciuria. The finding of the study needs to be confirmed by a large randomized trial in patient with PHPT and coexistent vitamin D deficiency
J Clin Endocrinol Metab 99: 1072– 1080, 2014) BMD increased in LS by 2. 4% prior to surgery (Vit D vs placebo)
Randomized, controlled study of Vit D treatment before and after surgery
Randomized, controlled study of Vit D treatment before and after surgery
J Clin Endocrinol Metab 99: 1072– 1080, 2014)
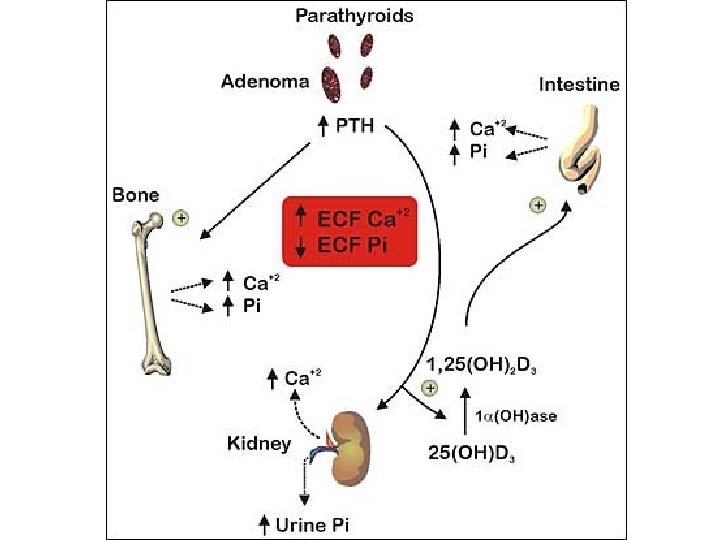
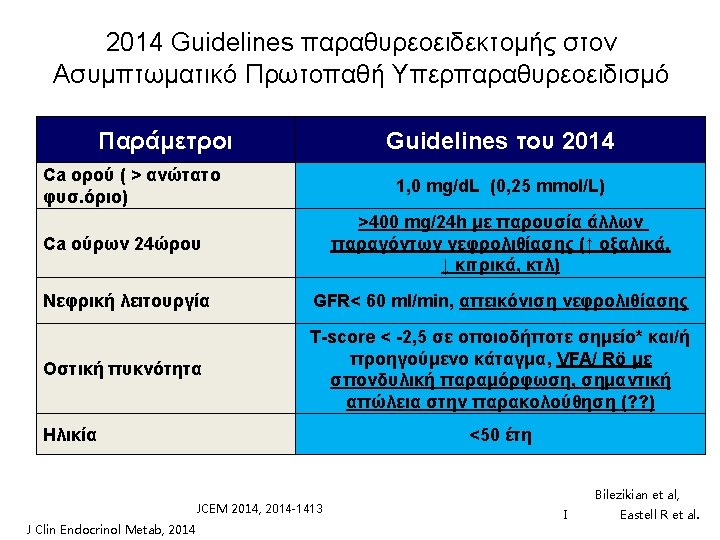
ΚΛΙΝΙΚΕΣ ΕΚΔΗΛΩΣΕΙΣ ΠΡΩΤΟΓΕΝΟΥΣ ΥΠΕΡΠΑΡΑΘΥΡΕΟΕΙΔΙΣΜΟΥ 1. Asymptomatic hypercalcemia detected by routine biochemical screening 2. Symptomatic hypercalcemia 3. During evaluation for manifestations of hyperparathyroidism such as osteopenia, osteoporosis, or nephrolithiasis 4. Rarely, hyperparathyroid bone disease (osteitis fibrosa cystica) or parathyroid crisis
Symptoms and signs of excess parathyroid hormone secretion • • • Symptoms and signs of hypercalcemia Bone disease Nephrolithiasis Hypophosphatemia Increased production of calcitriol Proximal renal tubular acidosis Hypomagnesemia Hyperuricemia and gout Anemia
Η ΜΟΝΤΕΡΝΑ ΚΛΙΝΙΚΗ ΕΙΚΟΝΑ ΤΟΥ ΠΡΩΤΟΓΕΝΟΥΣ ΥΠΕΡΠΑΡΑΘΥΡΕΟΕΙΔΙΣΜΟΥ Cope et al. 19301965 Nεφρολιθίαση Heath et al. Mallette et 1965 -1974 al. 1965 -1974 Silverberg, Bilezikian et al. 1984 -2006 57% 51% 37% 17% Not reported 36% 40% 39% Εμφανής σκελετική νόσος 23% 10% 14% 1. 4% Ασυμπτωματικός 0. 6% 18% 22% 80% Υπερασβεστιουρία Silverberg SJ and Bilezikian JP (2006)
Η βιοχημική εικόνα του πρωτογενούς υπερπαραθυρεοειδισμού στην μοντέρνα εποχή Παράμετρος Τιμές Ασθενείς Φυσιολο. • Calcium (mg/dl) 10. 7± 0. 1 8. 4 -10. 2 • Phosphorus (mg/dl) • Alk Phos (IU/l) 2. 9± 0. 1 114± 4 2. 5 -4. 5 <100 • PTH (pg/ml) 121± 7 10 -65 • • 21± 1 59± 2 248 + 12 17 + 6 9 -52 15 -60 100 -300 4 -21 25 -OH Vit D (ng/ml) 1, 25 -OH 2 Vit D (pg/ml) Urinary calcium (mg) DPD (nmol/mmol Cr) Silverberg, Bilezikian et al.
Bone Mineral Density: % of Expected Η οστεοπυκνομετρική εικόνα του πρωτογενούς υπερπαραθυρεοειδισμού στην μοντέρνα εποχή 100 * * * Differs from ra p<. 05 90 80 70 Lumbar Spine Silverberg, Bilezikian et al. JBMR, 1989 Femoral Neck Radius
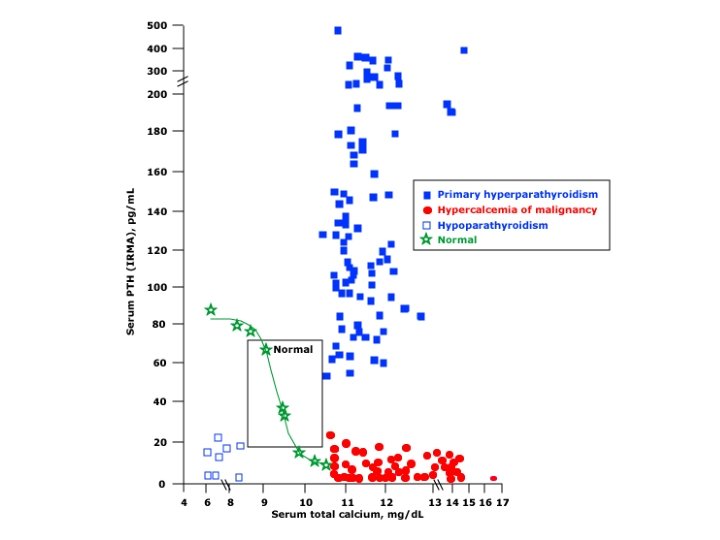
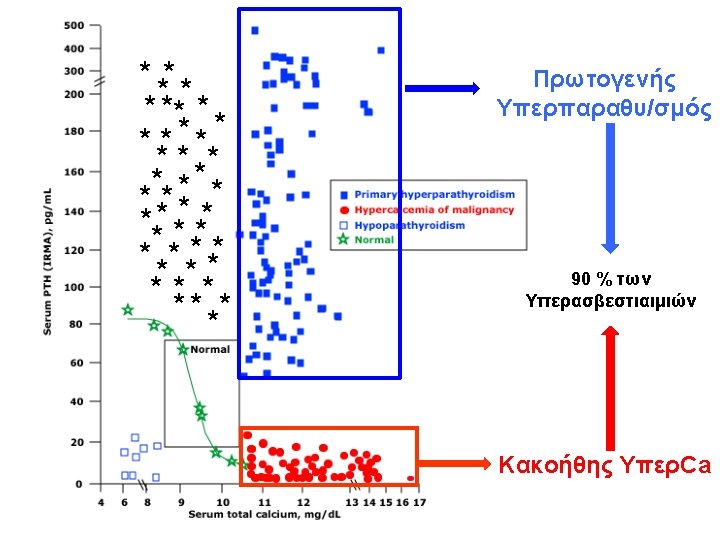
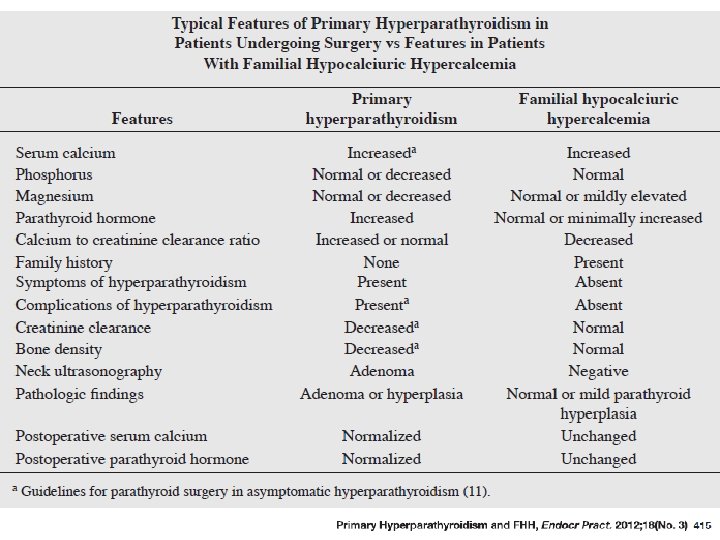
Differential diagnosis of primary hyperparathyroidism, typical laboratory findings 90%
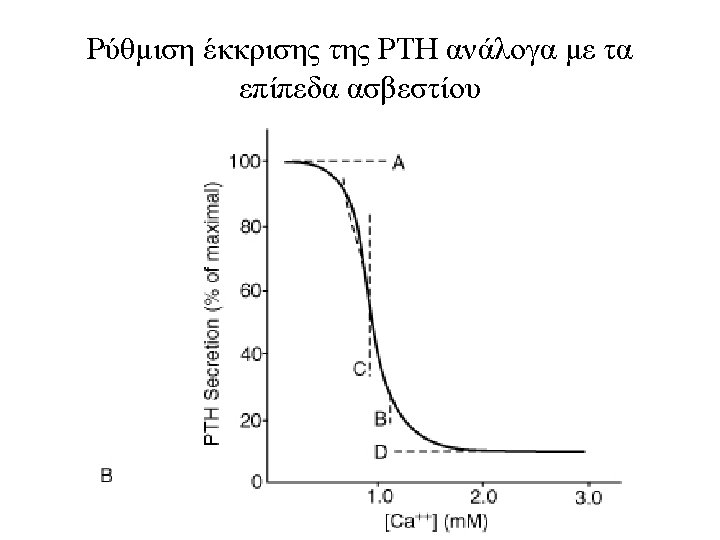
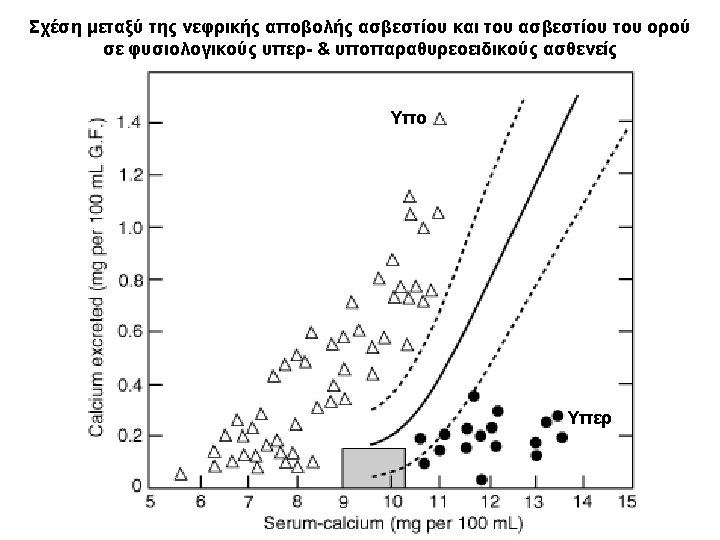
Serum calcium concentration vs serum intact parathyroid hormone
FHH versus PHPT, Endocr Pract. 2013; 19(No. 4)
Κλασματική απέκρισση Ca Ca/Cr clearance ratio = [24 -hour Urine Ca x serum Cr] ÷ [Serum Ca x 24 hour Urine Cr] The ratio of calcium (Ca) clearance to creatinine (Cr) clearance may be used for the diagnosis of FHH using the following formula: Cl Ca/ Cl Cr = (Cau x Crs)/Cru x Cas) where Cau = urinary Ca concentration, Crs = serum Cr concentration, Cru = urinary Cr concentration, and Cas = serum Ca concentration. A ratio of 0. 01 or less is typically seen in individuals with FHH.
Diagnostic approach to hypercalcemia
A 21 -yr old man with a calcium level of 15. 2 mg/dl. Eight weeks earlier he had sustained multiple broken bones, a left nephrectomy, and a colostomy due to a motor vehicle accident. Despite rapid recovery, wellhealed surgeries, and a normal glomerular filtration rate, the patient remained in bed on narcotics for generalized discomfort. Importantly, his PTH was suppressed. The Endocrine team made the following simple recommendation: get the patient to stand Up. Clin Endocrinol Metab, May 2010, 95(5): 2050– 2053
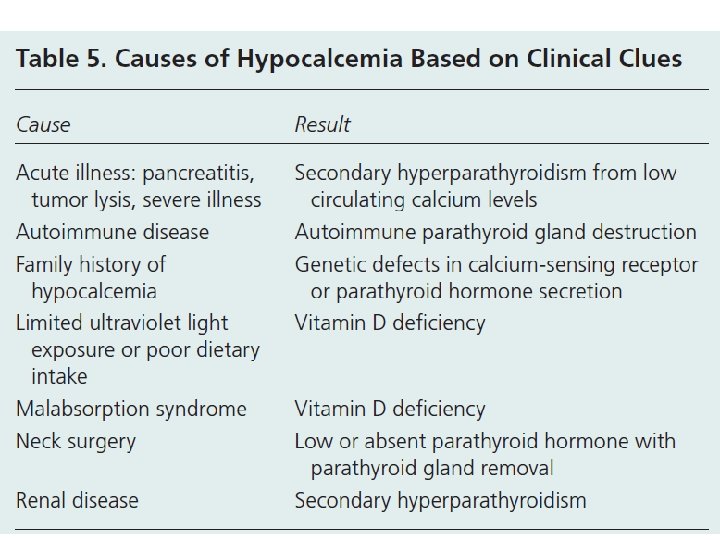
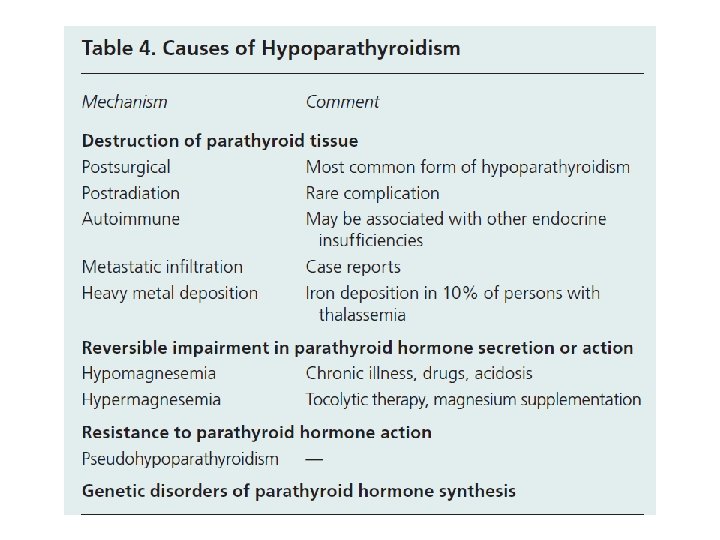
Causes and mechanisms of hypocalcemia Curr Opin Nephrol Hypertens 2013, 22: 371– 376
Causes of hypocalcemia
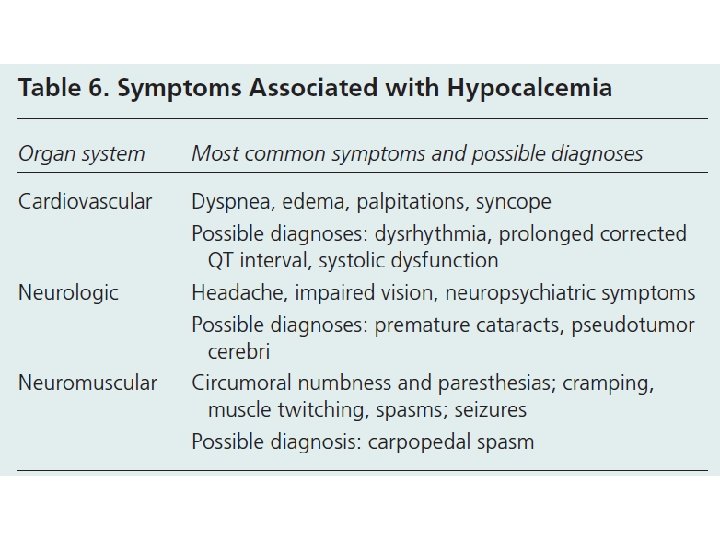
Clinical manifestations of hypocalcemia Prolonged QT interval due to hypocalcemia
Hypocalcemia Basic investigations to establish a specific diagnosis, along with more specialized tests that might be required in specific cases Basic investigations • Serum calcium (corrected) • Phosphate • Magnesium • Electrolytes • Creatinine • Alkaline phosphatase • Parathyroid hormone • 25 -hydroxyvitamin D • Serum p. H • Complete blood count Further investigations • Ionized calcium • 24 -hour urinary phosphate, calcium, magnesium, and creatinine • 1, 25 -dihydroxyvitamin D • Renal ultrasonography to assess for nephrolithiasis • DNA sequencing to exclude genetic mutations • Biochemistry in first-degree family members
Biochemical manifestations of different stages of vitamin D deficiency, as compared with deficiencies of calcium or phosphorus
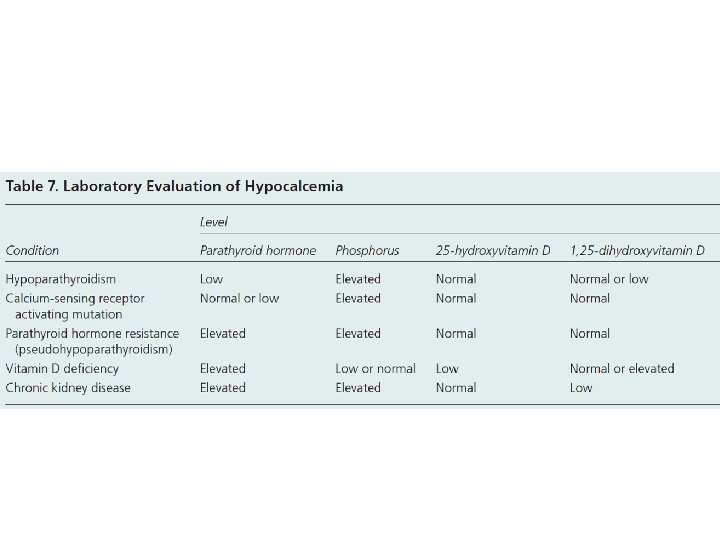
Evaluation of Hypocalcemia
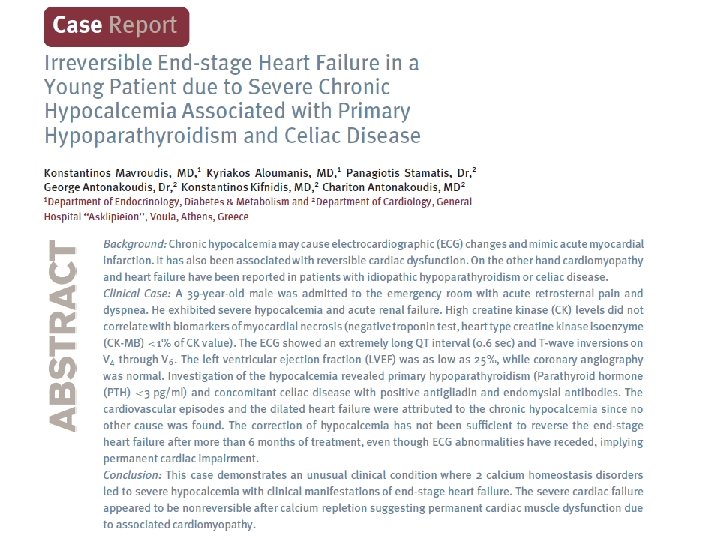
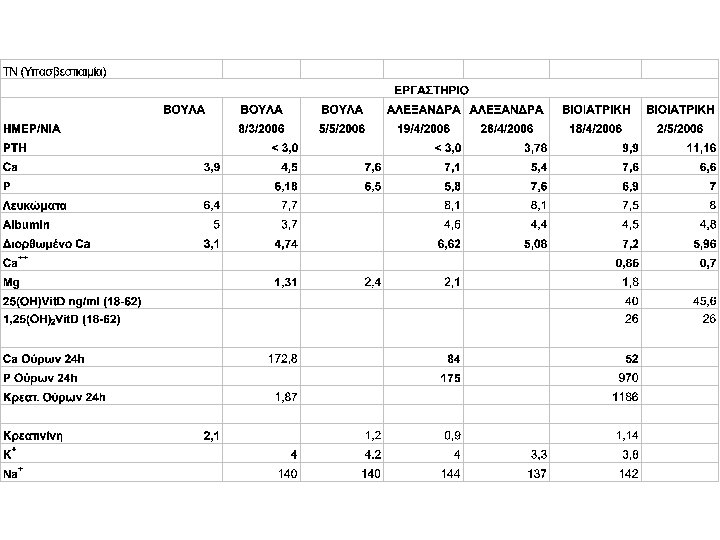
• W. B. C 7. 910 / u. L. , Neu 76 %, Lymph. . 8 %, Mono 15 %, Ht 32. 1 %, M. C. V. 74. 6 f. L, M. C. H. 22. 9 pg, P. L. T. 378. 000 /u. L, Σάκχαρο 117 mg/dl, Ουρία 65 mg/dl, Κρεατινίνη 2. 1 mg/dl, Αμυλάση 141. U/L, Ολ. Χολερυθρίνη 0. 3 mg/dl, Χοληστερίνη 104 mg/dl, Τριγλυκερίδια 68 mg/dl, Ολ. Λευκώματα 6. 4 g/d. L, Αλβουμίνη 5. 0 g/d. L, Ουρικό οξύ 8. 9 mg/d. L , SGOT 63 U/L, SGPT 58 U/L, ALP 69 U/L, γGT 36 U/L, LDH 521 U/L, Na 139 mmol/L, K 3. 0 mmol/L, Ca 3, 9 mg /dl • Αέρια αίματος : p. H 7. 36, p. CO 2 23 mm Hg, p. O 2 120 mm Hg ( με μάσκα Venturi ), HCO 3 13 mmol / L, Lact 10. 7 mmol / L, • SO 2 : 99 %, Σάκχαρο 243 mg / dl
Λαμβανόμενη Φαρμακευτική Αγωγή πριν την εισαγωγή -Lopresor 100 mg tb. ½x 2 -Imdur 60 mg tb. 1 x 1 -Lasix 500 mg tb. 1/2 x 1 -Lipitor 40 mg tb. 1 x 1 -Salospir 100 mg tb. 1 x 1 -Zofepril 30 mg tb. ½x 1 -Tarontal 400 mg tb. 1 x 1
Φαρμακευτική αγωγή κατά τη νοσηλεία του : -Clexane 80 mg 1 x 2 -Salospir 100 mg tb 1 x 1 -Plavix 75 mg tb 1 x 1 -Lasix 20 mg amp 2 x 2 -Dilatrend 6. 25 mg tb ½x 2 -Zestril 5 mg tb 1 x 1 -Lexotanil 3 mg tb 1 x 1 -Losec 20 mg amp 1 x 1 -Integrilin (αναστολέας γλυκοπρωτείνης IIb/IIIa ) amp με ροή έγχυσης 18 ml/h
Management of Normo. Calcaemic PHPT JCEM 2014, 99: 3561
Different serum PTH assays in patients with primary hyperparathyroidism
Different serum (PTH) assays in patients with hypercalcemia of malignancy