Hypercalcemia 1 1 2 3 4 5 6




















 is a rare disease characterized by: • accumulation")


- Slides: 72
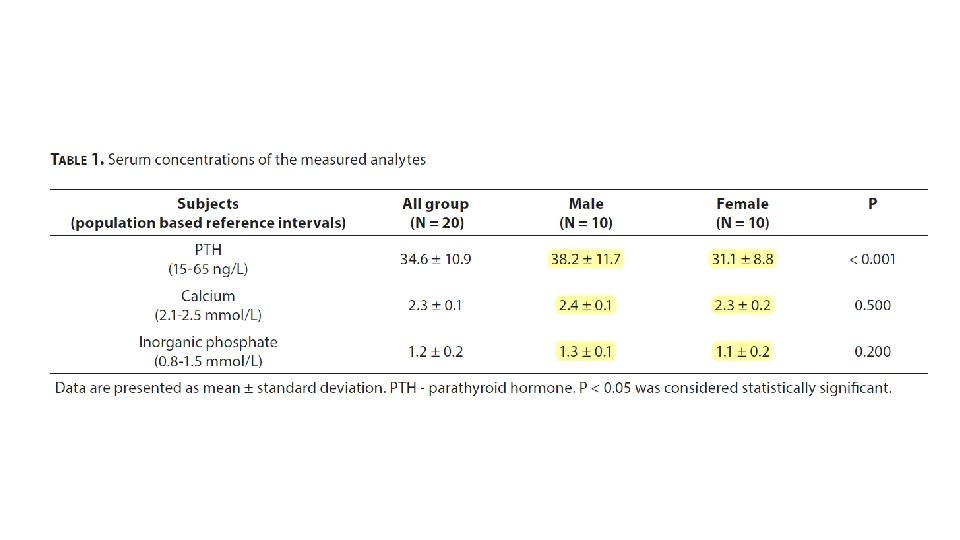
Hypercalcemia
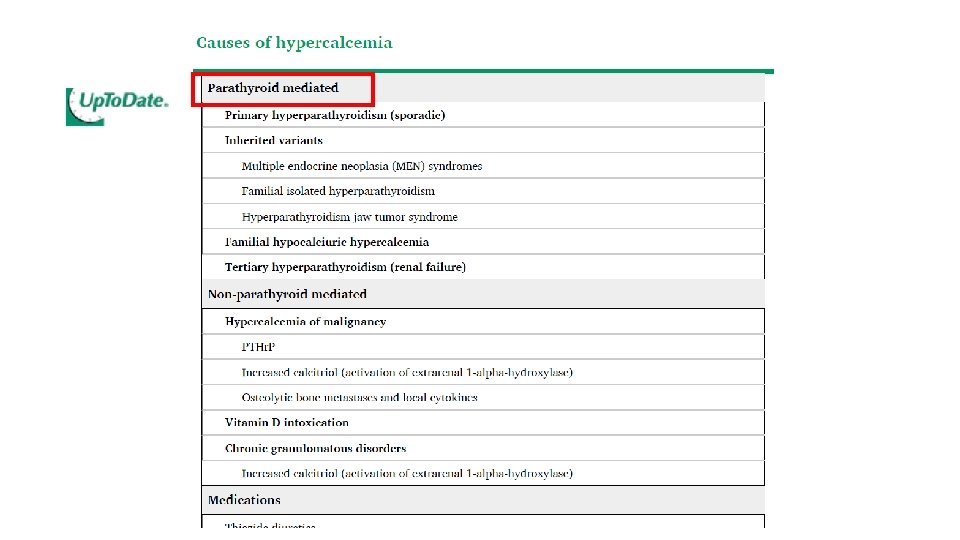
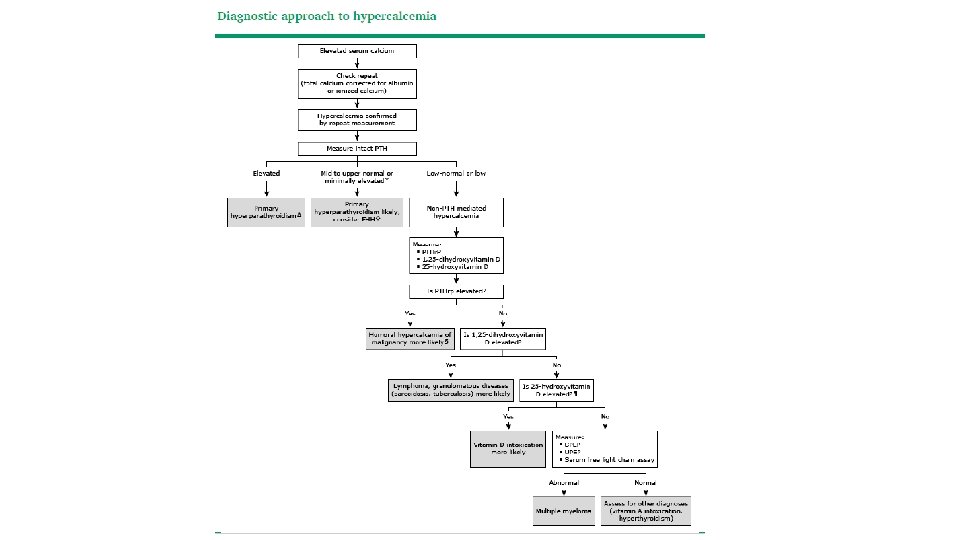
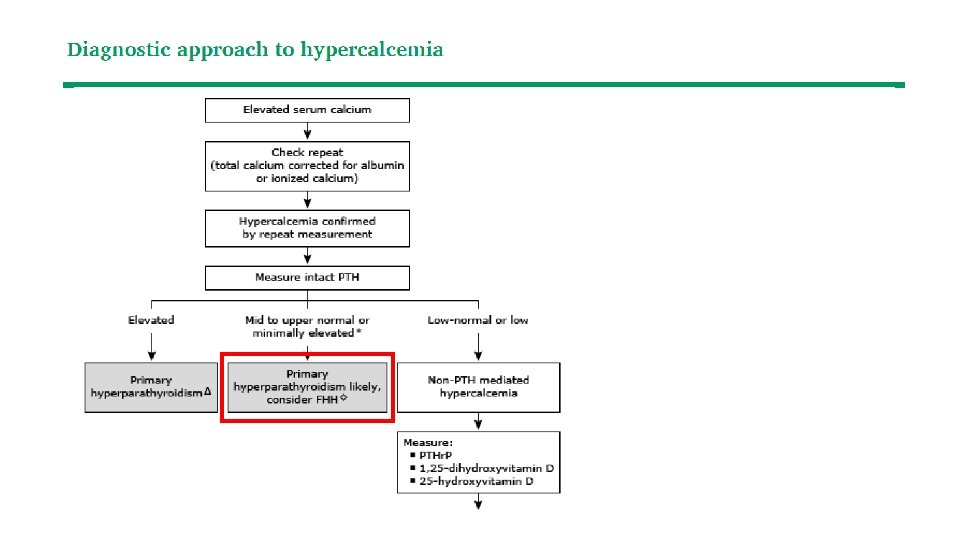
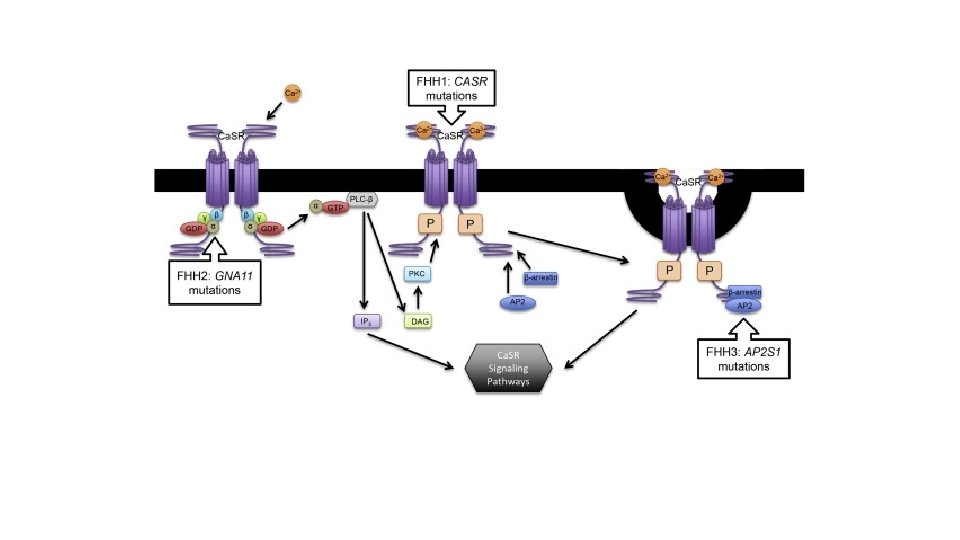
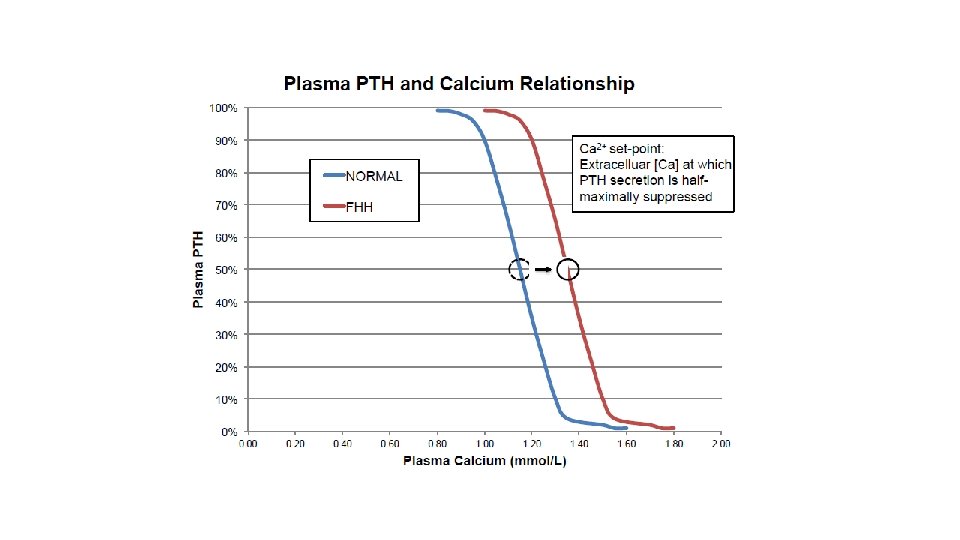
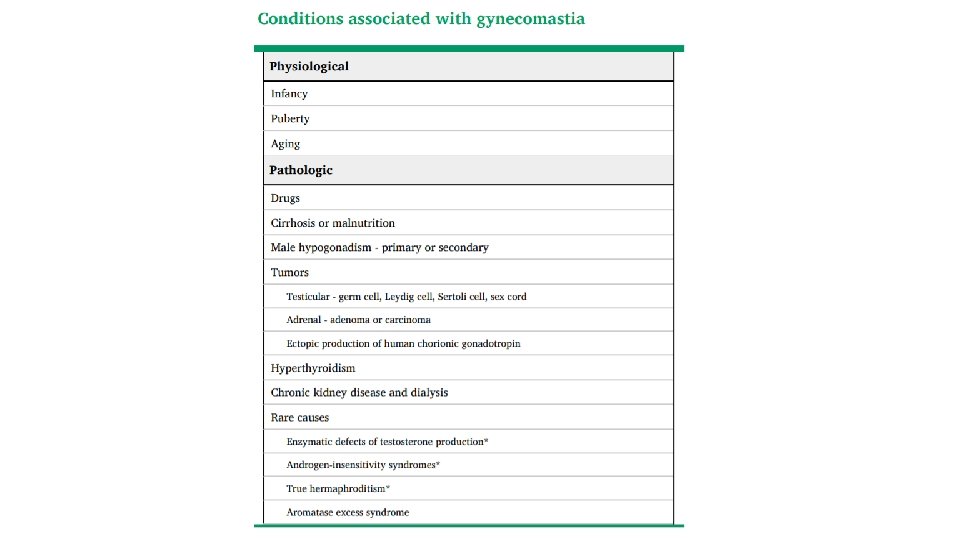
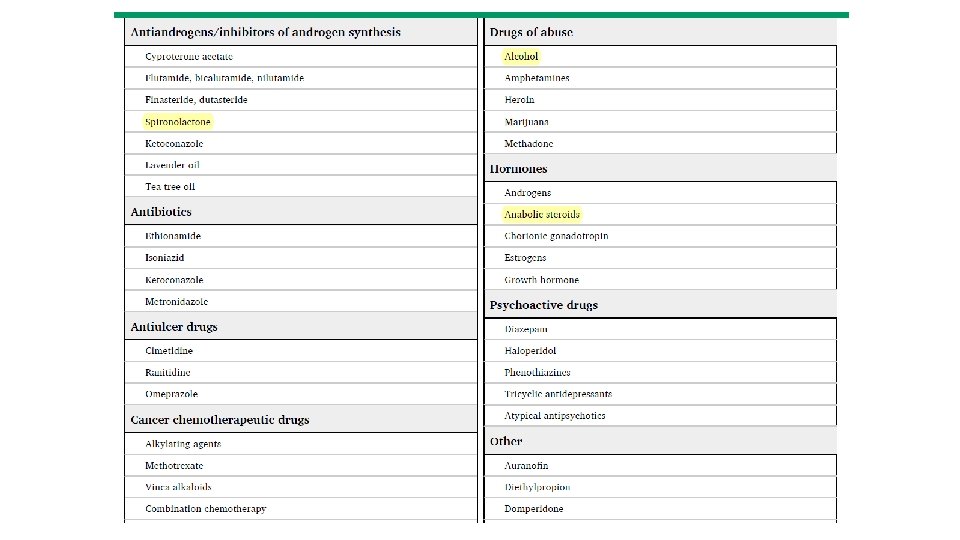
1 1 2 3 4 5 6 7 8 9 Primary or secondary HTN? What is the probable cause of hypercalcemia in this patient? Is there any variation in PTH level in serum? Primary hyperparathyroidism or FHH? Is urinary calcium excretion useful for diagnosis? What about manifestations in our patient? What is the utility of sestamibi scan? What is the probable type of hyperparathyroidism in the patient? 10 What is the etiology of gynecomastia? 11 Could hyperparathyroidism be the cause of hypertension in our patient?
1 1 2 Primary or secondary HTN? What is the probable cause of hypercalcemia in this patient? 3 Is there any variation in PTH level in serum? 4 Primary hyperparathyroidism or FHH? 5 6 7 8 9 Is urinary calcium excretion useful for diagnosis? What about manifestations in our patient? What is the utility of sestamibi scan? What is the probable type of hyperparathyroidism in the patient? 10 What is the etiology of gynecomastia? 11 Could hyperparathyroidism be the cause of hypertension in our patient?
1 1 2 Primary or secondary HTN? What is the probable cause of hypercalcemia in this patient? 3 Is there any variation in PTH level in serum? 4 Primary hyperparathyroidism or FHH? 5 6 7 8 9 Is urinary calcium excretion useful for diagnosis? What about manifestations in our patient? What is the utility of sestamibi scan? What is the probable type of hyperparathyroidism in the patient? 10 What is the etiology of gynecomastia? 11 Could hyperparathyroidism be the cause of hypertension in our patient?
1 1 2 Primary or secondary HTN? What is the probable cause of hypercalcemia in this patient? 3 Is there any variation in PTH level in serum? 4 Primary hyperparathyroidism or FHH? 5 6 7 8 9 Is urinary calcium excretion useful for diagnosis? What about manifestations in our patient? What is the utility of sestamibi scan? What is the probable type of hyperparathyroidism in the patient? 10 What is the etiology of gynecomastia? 11 Could hyperparathyroidism be the cause of hypertension in our patient?
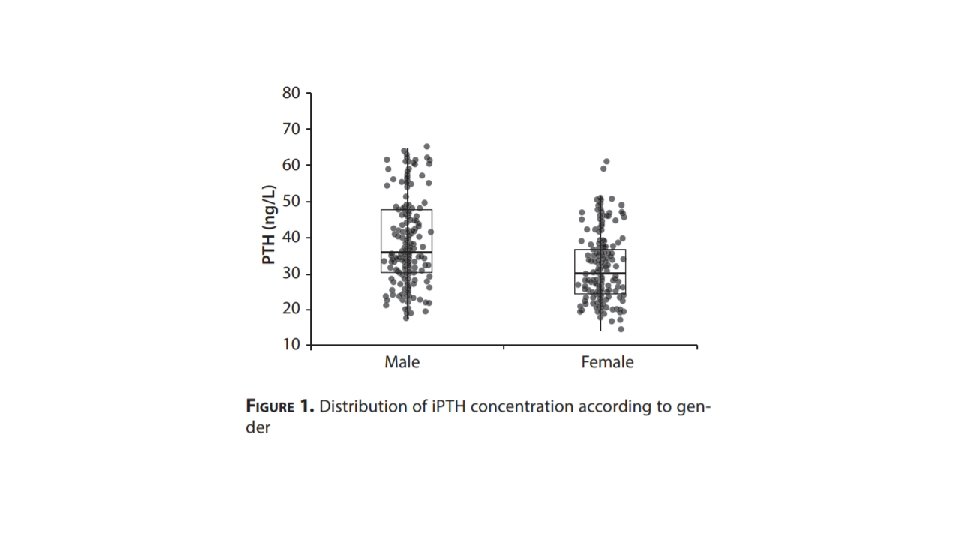
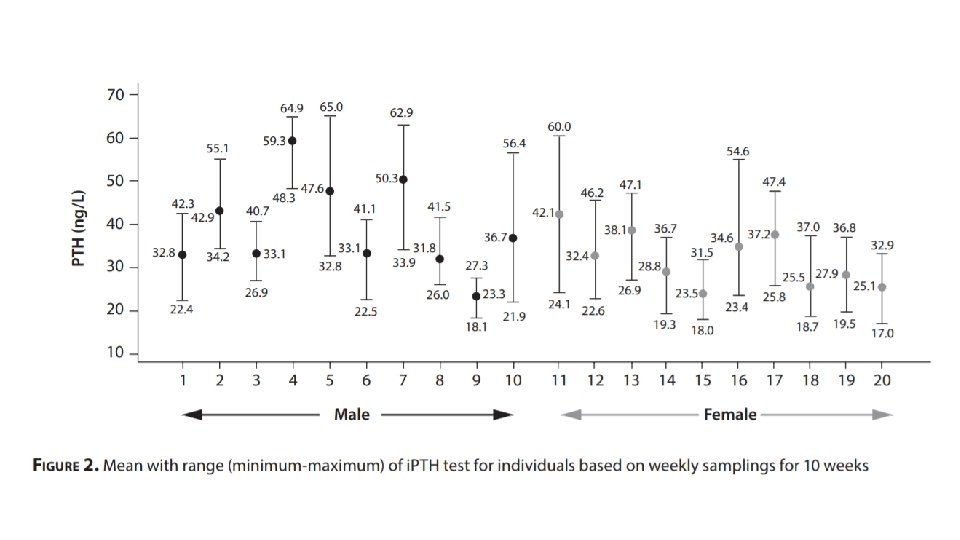
• Parathyroid hormone is secreted in three distinct ways: • tonic secretion • circadian dynamics (with the highest amount secreted in the morning and lowest in the evening) • a pulsatility that appears to be stochastic (occurring unpredictably, ten or more times a day). • Most parathyroid hormone is secreted continuously
1 1 2 Primary or secondary HTN? What is the probable cause of hypercalcemia in this patient? 3 Is there any variation in PTH level in serum? 4 Primary hyperparathyroidism or FHH? 5 6 7 8 9 Is urinary calcium excretion useful for diagnosis? What about manifestations in our patient? What is the utility of sestamibi scan? What is the probable type of hyperparathyroidism in the patient? 10 What is the etiology of gynecomastia? 11 Could hyperparathyroidism be the cause of hypertension in our patient?
0. 01 0. 02
1 1 2 Primary or secondary HTN? What is the probable cause of hypercalcemia in this patient? 3 Is there any variation in PTH level in serum? 4 Primary hyperparathyroidism or FHH? 5 6 7 8 9 Is urinary calcium excretion useful for diagnosis? What about manifestations in our patient? What is the utility of sestamibi scan? What is the probable type of hyperparathyroidism in the patient? 10 What is the etiology of gynecomastia? 11 Could hyperparathyroidism be the cause of hypertension in our patient?
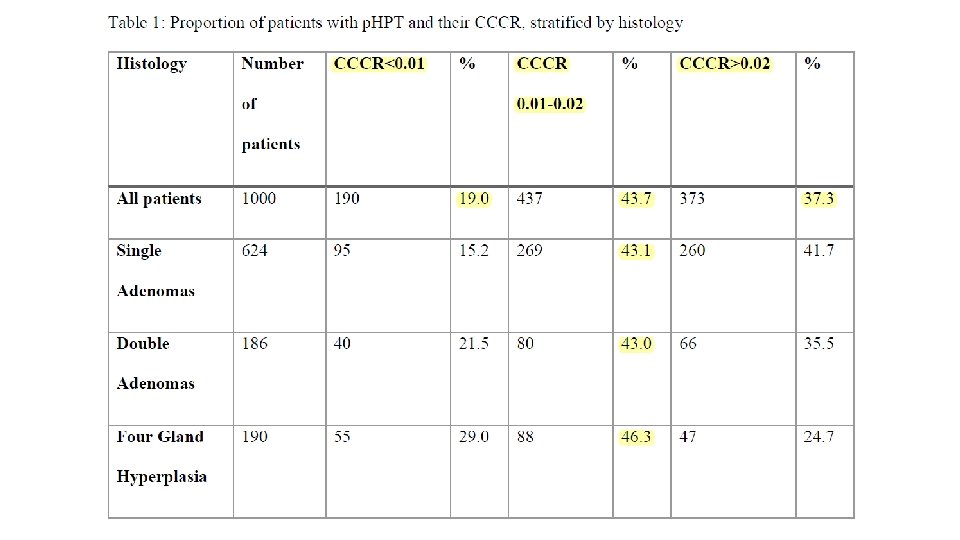
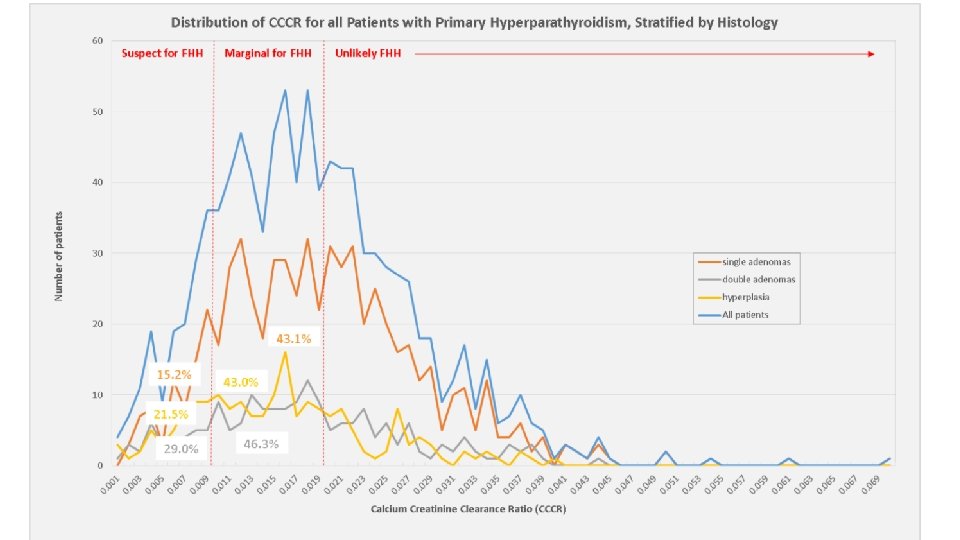
• retrospective study of 1000 patients who underwent parathyroid surgery for p. HPT over 11 years • CCCR was: • less than 0. 01 for 19. 0% • between 0. 01 -0. 02 for 43. 7% • greater than 0. 02 in 37. 3%.
1 1 2 Primary or secondary HTN? What is the probable cause of hypercalcemia in this patient? 3 Is there any variation in PTH level in serum? 4 Primary hyperparathyroidism or FHH? 5 6 7 8 9 Is urinary calcium excretion useful for diagnosis? What about manifestations in our patient? What is the utility of sestamibi scan? What is the probable type of hyperparathyroidism in the patient? 10 What is the etiology of gynecomastia? 11 Could hyperparathyroidism be the cause of hypertension in our patient?
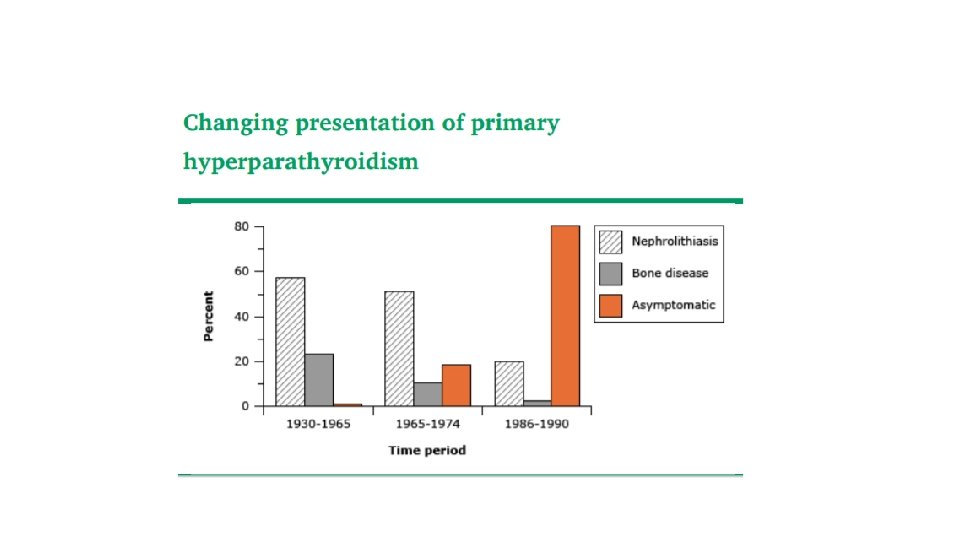
• USA and Canada : • primary hyperparathyroidism predominantly presents as an asymptomatic disorder. • Europe: • Similar to the epidemiology in North America, primary hyperparathyroidism in Europe most often presents as an asymptomatic disorder. • Asia • In Asia, primary hyperparathyroidism is more likely to present with more marked hypercalcaemia and target organ involvement than in other regions of the world.
Classical Features The Kidney: • Renal involvement can take the forms of : • • Hypercalciuria Nephrolithiasis Nephrocalcinosis reduced renal function • stones and/or nephrocalcinosisis actually present in 21% to 55% of patients with asymptomatic PHPT.
The bone • DXA is used to determine the advisability of surgery in asymptomatic patients. • Typically, bone loss is greatest at the forearm (33% radius), a skeletal site that is almost totally comprised of cortical bone, and least at the lumbar spine, a skeletal site with a large component of trabecular bone • Patients who do not have distal forearm measurements may have unrecognized but substantial cortical bone loss.
1 1 2 Primary or secondary HTN? What is the probable cause of hypercalcemia in this patient? 3 Is there any variation in PTH level in serum? 4 Primary hyperparathyroidism or FHH? 5 6 7 8 9 Is urinary calcium excretion useful for diagnosis? What about manifestations in our patient? What is the utility of sestamibi scan? What is the probable type of hyperparathyroidism in the patient? 10 What is the etiology of gynecomastia? 11 Could hyperparathyroidism be the cause of hypertension in our patient?
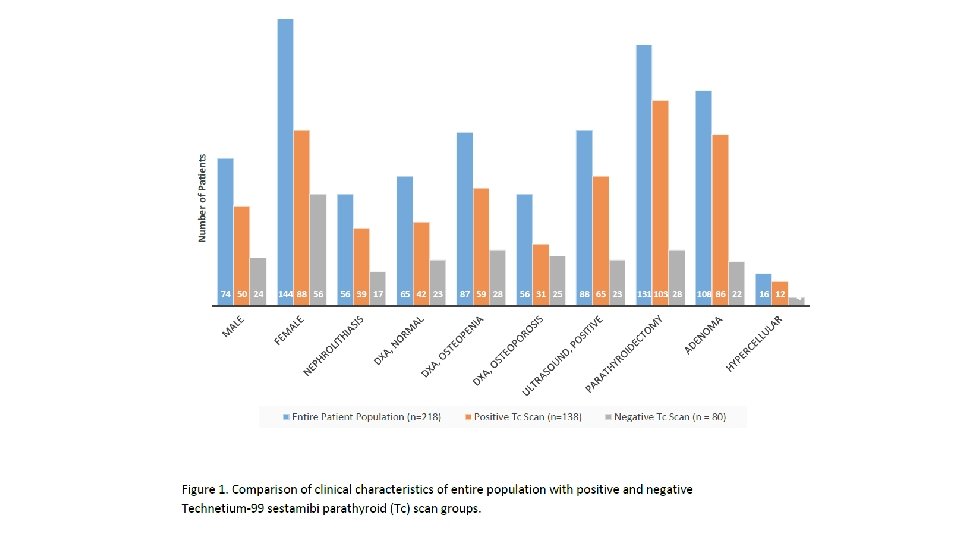
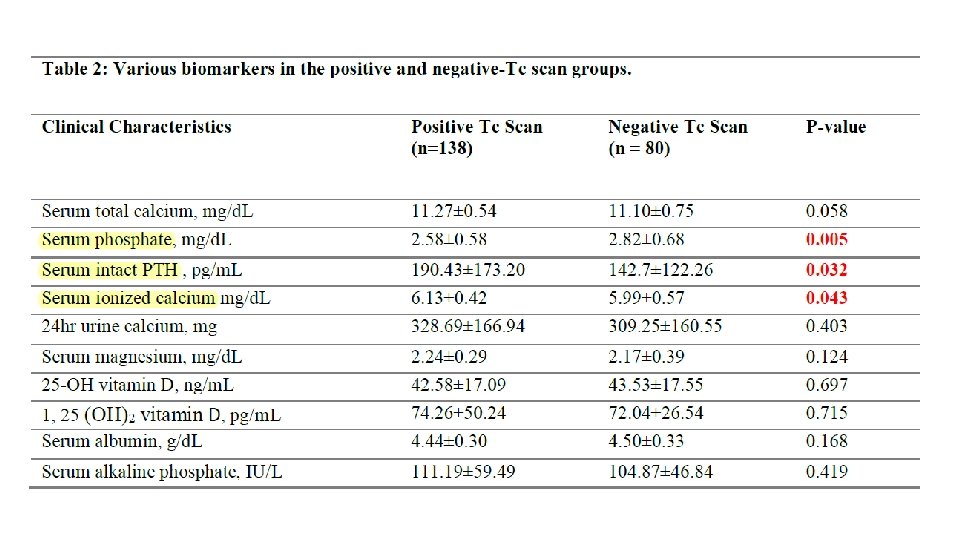
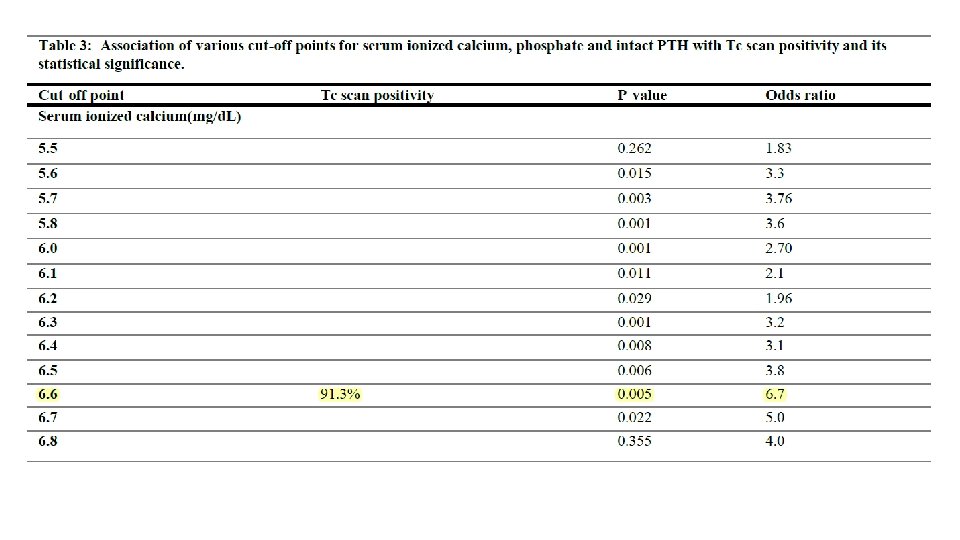
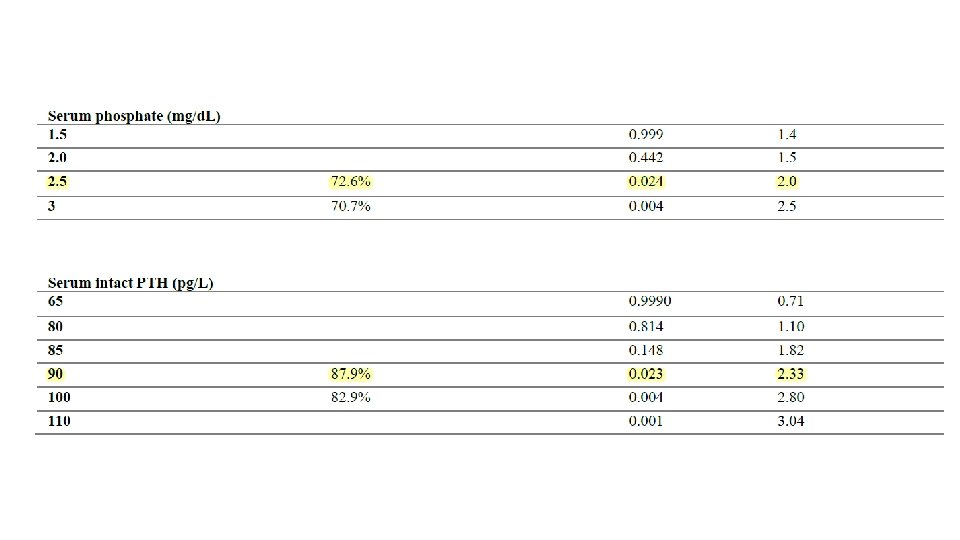
• Parathyroid Localization Modalities: What Imaging to Perform and When • Imaging has no utility in confirming or excluding the diagnosis of p. HPT. • Imaging results should not be used to select patients for surgical referral. • Patients with negative imaging results remain candidates for parathyroidectomy. • When imaging with initially negative results is performed again at high volume centers, the sensitivity of localization improves to as high as 92%. • Imaging is performed after deciding to proceed with parathyroidectomy and is performed for operative planning.
1 1 2 Primary or secondary HTN? What is the probable cause of hypercalcemia in this patient? 3 Is there any variation in PTH level in serum? 4 Primary hyperparathyroidism or FHH? 5 6 7 8 9 Is urinary calcium excretion useful for diagnosis? What about manifestations in our patient? What is the utility of sestamibi scan? What is the probable type of hyperparathyroidism in the patient? 10 What is the etiology of gynecomastia? 11 Could hyperparathyroidism be the cause of hypertension in our patient?
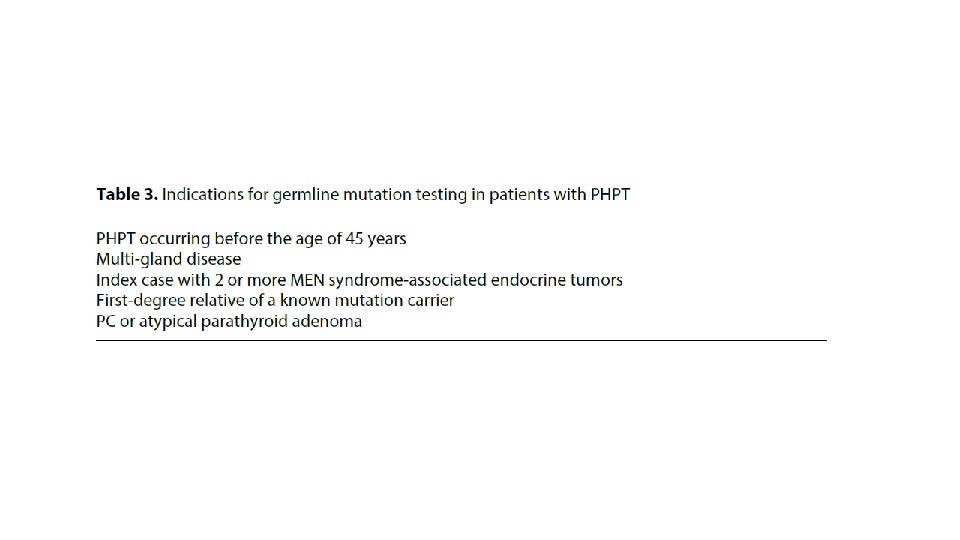
• Clinical management of a FPHPT proband his/her first-degree relatives • Apart from hyperparathyroidism evaluation , proband should undergo biochemical-clinical-radiological screening also for all the other possible associated functioning and/or non-functioning proliferative disorders, determining each specific syndrome. • when FPHPT is suspected, serum calcium measurement of first-degree relatives should be considered along with other clinical investigations
• First degree relatives of proband with suspect FPHPT • In these cases, sometimes normocalcemic PHPT is observed. • Thus • If the DNA test has revealed a causal germinal mutation in one of the genes responsible for FPHPT in the proband, then its identification in first-degree relatives is very helpful in clinical diagnosis confirmation, guiding both an appropriate medical management and timing of clinical biochemical follow-up in these subjects, specifically for each FPHPT syndrome
1 1 2 Primary or secondary HTN? What is the probable cause of hypercalcemia in this patient? 3 Is there any variation in PTH level in serum? 4 Primary hyperparathyroidism or FHH? 5 6 7 8 9 Is urinary calcium excretion useful for diagnosis? What about manifestations in our patient? What is the utility of sestamibi scan? What is the probable type of hyperparathyroidism in the patient? 10 What is the etiology of gynecomastia? 11 Could hyperparathyroidism be the cause of hypertension in our patient?
• Multiple symmetric lipomatosis (MSL) is a rare disease characterized by: • accumulation of unencapsulated fat, mainly located symmetrically around the neck, shoulders, and upper limbs. • Its etiology is still unknown; however, previous reports have shown that this disease is associated with alcoholism. Surgical intervention is the only effective treatment for this disease.
• The patient reported more than 20 years of alcohol abuse (about 500 g/d) and heavy smoking (about 20 cigarettes per day).
1 1 2 Primary or secondary HTN? What is the probable cause of hypercalcemia in this patient? 3 Is there any variation in PTH level in serum? 4 Primary hyperparathyroidism or FHH? 5 6 7 8 9 Is urinary calcium excretion useful for diagnosis? What about manifestations in our patient? What is the utility of sestamibi scan? What is the probable type of hyperparathyroidism in the patient? 10 What is the etiology of gynecomastia? 11 Could hyperparathyroidism be the cause of hypertension in our patient?