Guided Clinical Mentorship at Inspira Health Network Lynette






























- Slides: 33
Guided Clinical Mentorship at Inspira Health Network Lynette Newkirk, RN Administrative Director, Care Coordination & Patient Relations Inspira Health Network Michelle Wieczorek RN RHIT CPHQ General Manager, Coding and CDI Practice e 4 Services
Objectives § Review the decision making process of Inspira Health Network in selecting a hybrid model and approach to CDI. § Review the LEAN Six Sigma approach to implementing a CDI Program, including the use of an a 3. § Examine the Guided Clinical Mentorship Program for CDI Training. § Examine the program challenges, opportunities and achievements through use of a CDI Dashboard implemented to visualize and manage the workplan.
About Inspira § Inspira Health Network is a charitable nonprofit health care organization formed in November 2012 by the merger of South Jersey Healthcare and Underwood. Memorial Hospital. § The Network comprises three hospitals (Vineland, Elmer and Woodbury Campuses), four multi-specialty health centers and a total of more than 60 locations. § 1, 100 physicians and other health care providers provide evidence-based care to help each patient achieve the best possible outcome.
Michelle Wieczorek, e 4 GOING LEAN WITH CDI AND KEY DECISIONS
Key Program Drivers for Inspira § Prepare Providers for ICD-10 § Improve Medicare Performance Indicators • • LOS CC/MCC Capture Rates CMI PEPPER § Support Physician Engagement/Alignment Strategies such as Gainsharing § Strengthen Coding -“Audit Ready Record” § Leverage Existing Infrastructure-FTE Neutral
TOP 15 DRG Pairs/Triplets by Volume YTD: DECEMBER 31, 2014 CMI CC & MCC Capture Annual Volume Actual Bench Current Bench 629 1. 117 1. 168 80% 87% 35% 42% DRG Group 291_292_293 Group Name Heart failure & shock 190_191_192 Chronic obstructive pulmonary disease 509 1. 020 0. 996 82% 80% 48% 41% 308_309_310 193_194_195 Cardiac arrhythmia & conduction disorders Simple pneumonia & pleurisy 344 328 0. 857 1. 176 0. 829 1. 132 65% 85% 66% 88% 33% 45% 26% 34% 314 299 234 0. 812 1. 183 0. 900 0. 823 1. 214 0. 916 17% 91% 30% 19% 94% 34% 17% 30% 19% 42% 34% 228 2. 188 2. 285 7% 14% 226 224 1. 172 1. 119 1. 305 1. 178 68% 78% 81% 87% 20% 22% 36% 27% 205 0. 846 0. 819 37% 31% 193 180 1. 265 0. 947 1. 416 0. 962 66% 17% 81% 19% 39% 17% 54% 19% 165 135 1. 667 0. 928 1. 721 1. 034 73% 66% 80% 78% 73% 14% 80% 23%6 391_392 Esophagitis, gastroent & misc digest disorders 682_683_684 Renal failure 689_690 Kidney & urinary tract infections Major joint replacement or reattachment of 469_470 lower extremity Intracranial hemorrhage or cerebral 64_65_66 infarction 377_378_379 G. I. hemorrhage 640_641 Nutritional & misc metabolic disorders 280_281_282 Acute myocardial infarction, discharged alive 602_603 Cellulitis Septicemia or severe sepsis w/o MV 96+ 871_872 hours 388_389_390 G. I. obstruction e 4 Services LLC
CDI Schematic for Vineland Elmer CDI Program is Live SWOT February 24 -25 SWOT Debrief and Decision to Proceed with GCM March 4 LEAN Event March 1011 LEAN Debrief and Straw Model Alignment March 17 GCM Didactic (3 Days) GCM Program 10 Weeks Physician Education Didactic Sessions April May July January (Woodbury Focus) 7
Two Basic CDI Models HIM-Coding Based Nurse-Clinical Model RHIA’s/RHIT’s/CCS’s RN’s and LPN’s Concurrent and/or Retrospective (Pre. Bill) Concurrent Focus on Improved Documentation for Coding and DRG Assignment Focus on Improved Documentation for Diagnosis Clarity, Specificity and Capture of Acuity Record is concurrently coded and validated at Discharge Often have a Quality Focus (HAC’s, PSI’s and Core Measures) HYBRID Decreases DNFB/AR Impact Queries are often electronic, or paper based. Staff must be able to code-very challenging High reliance on encoder and other technology during reviews Reporting structure is variable but not usually to HIM Emphasis on VERBAL queries with a broad focus of query types (Severity, Medical Necessity and Quality Indicators in-play)
Executive Summary and Recommendations MARCH 2015 § A hybrid CDI Model is likely to be successful in a care management model at Vineland Elmer campuses. § Risks include Physician Engagement Strategy and Optimal Staffing to achieve a best practice CDI program. § A LEAN event will help to further clarify the process changes and technology augmentation that is required to fully execute the program, including a straw model review of the proposed CDI role. § Existing structures for the care management program can be leveraged today to produce the desired outcomes for the program. § e 4 recommends a thoughtful yet assertive timeline to achieve the best results in the current ramp up to ICD-10. • Move quickly to schedule the 10 Week GCM to get it established before summer vacations become problematic. • Conduct physician education on the heels of the GCM to leverage what has been observed during the initial learning period. 9
Day One-LEAN Event § 8: 30 AM-8: 45 AM Introductions and Welcome § 8: 45 AM-9: 15 AM Alignment on Goals and Objectives § 9: 15 -10: 00 AM Design Overview-CDI/Care Management Straw Model § 10: 00 AM-10: 15 AM Break § 10: 15 AM-12: 00 PM Inpatient Coding Current State Exercise with CDI Integration in Current and Future States § 12: 00 -12: 45 PM Lunch § 12: 45 PM-2 PM Concurrent Query Current State and Design Impacts on Future State § 2 PM-2: 15 PM Break § 2: 15 -4: 30 PM Concurrent Query Future State Alignment » Concurrent Query Gap Analysis » Verbal Query Practices » Electronic Queries 10
Day Two-LEAN Event § 8: 30 -9: 30 AM § 9: 30 -10: 45 AM • • • Review a 3 Drafts from Day 1 Physician Integration Current State and Future State Vision Peer Advisor Role Discussion Escalation Protocols (Delinquent Records, Abandoned Queries) Verbal Query Practices Documentation and Query Guideline Development Electronic, Verbal and Written Query Workflows § 10: 45 AM-11: 00 AM Break § 11: 00 AM-12: 30 PM CDI Dashboard Metrics-Future State » Available Metrics » Physician-Oriented Metrics » Technology Augmentation § 12: 30 PM-1: 15 PM Lunch § 1: 15 PM-3: 00 PM Guided Clinical Mentorship Impact Assessment and Workplan Adjustments § 3: 00 PM-3: 30 PM Adjournment/Next Steps 11
12
Straw Model
Lynette Newkirk, Inspira EXECUTING THE PROGRAM
Inspira Care Coordination Overview § Geographical & Physician Specific Care Coordinators • Discharge Planning, Progression of Care, UR review for Federal Payers, CDI. § Utilization Review Coordinators – Medicare Advantage programs, all Commercial programs, CDI § COACH team – Transitions of Care • Chronic disease management – Registered Nurses and Community Paramedics • Drug and Alcohol Abuse – Certified Drug and Alcohol Counsellors § MSW • High Risk Discharge Planning
Consensus - Approach § Go fast § Go enterprise wide • (Woodbury had existing CDI Program that ultimately disbanded in lieu of new Care Management CDI Approach) § Train ALL 45 FTE’s in Care Management on CDI to Integrate into Role § Blend HIM FTE’s into program (FTE’s allocated to commercial payers)
GCM Content 5 Modules
e 4 Services LLC 18
Program Stakeholders and Governance § Inspira Steering Oversight Committee • Program Oversight • CFO, CPO, COO, Director Corporate Compliance, Director HIM, Administrative Director Care Coordination § e 4 , CC, HIM Steering Group • Operations, Tools, Techniques, Training • Coding and HIM Impact § Care Coordination Departments • Practice and Subject Matter Expertise Issues • Woodbury Director & Vineland Manager &Social Work Director
Visualize the Workplan
Task View of Each Area of Work Plan are Visible
Make it Work. Physician Engagement § Physician Training • • • Medical Staff Dept. meetings, office practices, elbow to elbow Train Hospitalist Team UR Committee Meeting , Gain Sharing Meeting
Make it Real. Operations Impact § Operationalize the efforts: • • 7 day per week Care Coordination 24/7 ED Coverage § Queries are permanent part of medical record ( ICD-10): • § Front load the process: • • ED CC – assign Principle Diagnosis Assign Working DRG § Daily Physician Led Interdisciplinary Rounds: • • CC documents clinical catches in CDI worksheet embedded in Soarian Visible to all who access record § Huddles Daily and Weekly • • • Care Coordinators CDI Coding • • • e 4, Corporate Compliance , CC, and Coding Supervisors included in development Physician does not have to double document Physicians are expected to complete real time ( tracking compliance) Accessible for Coders § CDI Tracker in Share Point • • • Process metrics and productivity Query Response Rate DRG Impact
CDI Impact Tool and Tracker
Michelle Wieczorek, e 4 and Lynette Newkirk, Inspira IMPACTS AND OPPORTUNITIES
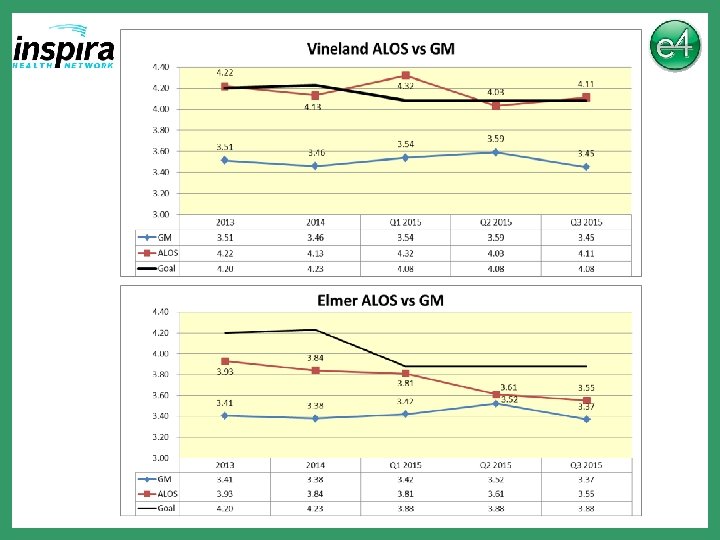
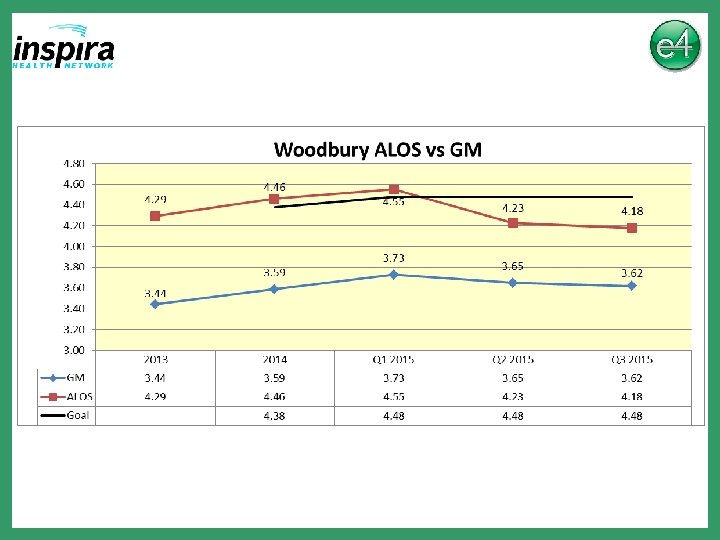
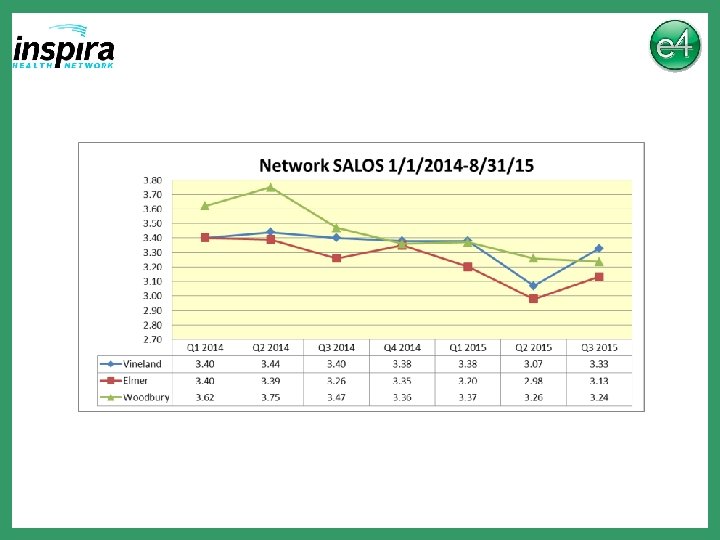
Average Length of Stay YTD and Goals ALL PAYER Campus YTD 12/31/14 LOS Goal LOS 2014 YTD 9/21/15 LOS Goal LOS 2015 Vineland 4. 13 4. 23 4. 15 4. 08 Elmer 3. 84 4. 23 3. 70 3. 88 Woodbury 4. 46 4. 38 4. 43 4. 48 Medicare Campus YTD 12/31/14 LOS YTD 9/21/15 LOS Goal LOS 2015 Vineland 5. 08 4. 81 4. 93 Elmer 4. 41 4. 11 4. 47 Woodbury 5. 22 4. 99 5. 32
• Woodbury is only June and July for 2014
• • 2015 Network Goal is 1. 45% % of Net Rev includes IP/OP
Work In Progress § 4 th GCM will Commence in Q 1 2016 § DRG Reconciliation Process Improvements • Physician Escalation Protocol § APR DRG’s § Improved Trackers • Single Solution-Multi User
THANK YOU FOR YOUR ATTENTION