Guided Tissue regeneration and Guided Bone Regeneration Guided
 is a method")
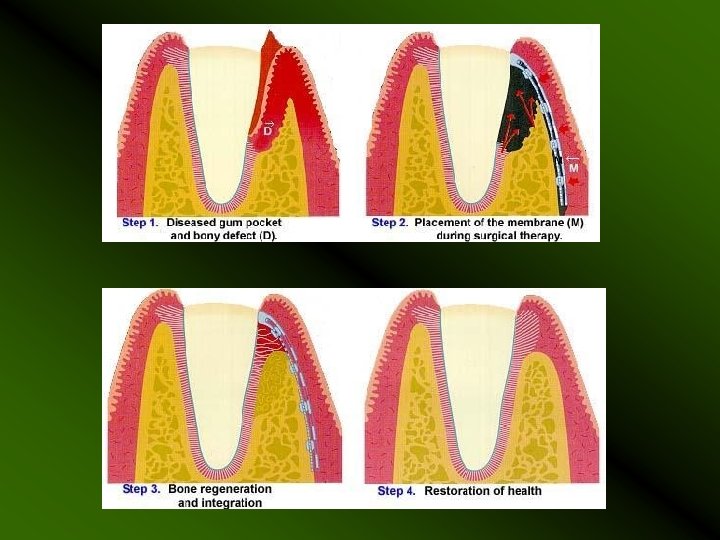
Guided Tissue regeneration and Guided Bone Regeneration Guided Tissue Regeneration (GTR) is a method for prevention of epithelial migration along the cemental wall of the pocket. Guided Bone Regeneration (GBR) is a procedure in which a membrane is placed over the bone defect site. This membrane encourages new bone to grow and also prevents the in-growth of fibrous scar tissue into the grafted site.

PRINCIPLE: Assumption that only periodontal ligament cells have the potential for regeneration of the attachment apparatus of the tooth. Exclusion of faster growing epithelium and connective tissue from the periodontal wound fro 6 to 8 weeks allows the slower growing tissues to occupy the space adjacent to the tooth. GTR The periodontal ligament cells and the cementoblasts are allowed to proliferate. GBR The osteoblasts are allowed to proliferate.

GUIDED TISSUE REGENERATION

INDICATION OF GTR *Class II Furcation lesion In Mandibular Molars And Interproximal Defects. *Peripheral Inflammatory Root Resorption – after surgical removal of granulation tissue.

*Treatment of periodontal pockets. *Recession-type defects *For pre-implant and peri-implant surgery

IDEAL PROPERTIES OF THE MEMBRANE: 1. Biocompatible 2. Space maintenance 3. Cell occlusiveness 4. Good handling properties 5. Resorbablity
 expanded polytetrafluoroethylene")
TYPES Non Resorbable : Milipore polytetrafluoroethylene ( Gore-Tex , Gore-Tex periodontal membrane) expanded polytetrafluoroethylene Resorbable : rat , bovine, porcine collagen cargile membrane - cecum of ox, polylactic acid Vicryl ( polyglactin 910) Biobrane Osseo. Quest – polyglycolic acid, polylactic acid, trimethylene carbonate – 6 – 14 months Bio. Guide- bilayer porcine derived collagen Atrisob- polylactic acid gel Bio. Mend- bovine Achilles tendon collagen – 4 to 18 weeks

Non - Resorbable membrane: Advantage: * Has the ability to maintain separation of tissues over an extended period of time. Disadvantage: • Require a second procedure to remove It, usually 3 to 6 weeks. * Early removal result in less bone regenration. *If it is exposed , will not heal spontaneously – can become contaminated with oral bacteria – infection-result in bone loss.


Resorbable Membranes Advantage: *Elimination of surgical re entry for the membrane removal. Disadvantage: *They can degrade before the bone formation is complete *Degradation process is associated with various degree of inflammation. *They are quite pliable- collapse of membrane into the defect area.

PROCEDURE: Raise the mucoperiosteal flap – minimum 2 teeth anteriorly, one tooth distally Debride the osseous defect and thoroughly plane the roots

Trim the membrane with sharp scissors to the approximate size. The borders of the membrane should extend 3 -4 mm apical to the margin of the defect, 2 -3 mm laterally beyond the defect, occlusally 2 mm apical to cemento enamel junction.

Suture the membrane tightly around the tooth – sling suture Suture the flap back in its original position. The flap should cover the membrane completely. Periodontal dressing maybe used. Antibiotic treatment is given to the patient for one week.

After 4 -6 weeks – margin of membrane is exposed. The membrane is removed with a gentle tug. If it cannot be removed – tissues are anaesthetized, and the material is removed surgically using a mini flap.

GTR IN POCKET THERAPY 21 with 10 mm pocket depth and 11 mm CAL. A midline diastema is present. Full thickness buccal and palatal flaps have been raised an intra bony defect can be seen. Modified Papilla Preservation Technique

A Ti reinforced e-PTFE barrier membrane has been placed and fixed close to the level of the CEJ. The membrane is completely covered. Primary closure has been obtained by preserving the interdental papilla and by the coronal displacement of the buccal tissue flap.

At 6 weeks the membrane is completely covered by healthy tissue. After membrane removal at 6 weeks , dense newly formed tissue is evident in the defect and in the supra crestal space maintained by the Ti – reinforced membrane

The newly formed tissue is completely covered by the raised and well preserved tissue flaps The photograph after 1 year shows a 4 mm residual pocket depth. A gain of clinical attachment of 6 mm was recorded and no recession has occurred compared to the baseline.

Recession Coverage using GTR
 using a membrane and bone graft. Initial")
GTR Case 2 Guided tissue regeneration (GTR) using a membrane and bone graft. Initial probing pocket depth: 11+ mm Final probing pocket depth: 4 mm at 10 months post-op Surgery by : Dr. Ricardo Diaz
 using a membrane and bone graft. Beginning")
GTR Case 3 Guided tissue regeneration (GTR) using a membrane and bone graft. Beginning probing pocket depth: 12+mm Final pocket probing depth: 4 mm at 12 months post-op Surgery by : Dr. Eduardo Lorenzana

ORTHODONTICS AND GTR In theory GTR is advantageous in orthodontic treatment for • Extrusion and Intrusion of teeth wit infra bony defect • Uprighting of tipped molars with mesioangular lesion • Pre orthodontic GTR can prevent the epithelium migrating apically and a bodily tooth movement into or through an intra bony defect can eliminate the bony pocket more easily. /

GUIDED BONE REGENERATION In the GBR technique, a barrier membrane is placed over the periodontal defect to prevent the in-growth of cells from the gingival connective tissue, epithelium, and the periodontal ligament.

INDICATION FOR GBR Periodontal defect Defects Around Dental Implants Defects Following Cyst or Tumor Surgery Insufficient Amount of Jaw Bone to Support Dentures or Bridges Defects Following Tooth Extraction

MATERIALS USED FOR GBR: Barrier Membrane: Resorbable Copolymers of polylactide and polyglycolide Collagen Non resorbabale Latex Teflon (e. PTFE) Titanium reinforced membrane – don’t need bone grafts for regenerating bone.

Bone grafts: Autografts Allografts Undecalcified freeze Dried Bone Allograft Decalcified Freeze Dried Bone Allograft Xenografts Boplant – calf bone Kiel Bone (calf or ox bone) Anorganic Bone – from ox Bio Oss ( Osteo health) – anorganic bovine derived bone They help in maintaining space under the barrier membrane to facilitate the formation of bone within a confined space. Requirement of Bone graft. They should facilitate the ingrowth of neo vascularisation and migration of osteoblasts.

BIOLOGICAL MECHANISMS OF BONE GRAFT MATERIALS Osteoconduction – formation of bone by osteoblasts from the margins of the defect on the bone graft material. Osteoconductive materials serve as scaffold for bone growth. Osteoinduction- new bone formation through the stimulation of osteoprogenitors from the defect to differentiate in to osteoblasts and begin new bone formation. Osteogenesis- occurs when living osteoblasts are part of the bone graft , as in autogenous transplantation.

The following is one example of these procedures following tooth extraction. 1. The tooth is removed and the remaining tooth socket is thoroughly cleaned of all inflamed and infected tissue. 3. GBR membrane (eg. Bio. Gide®) is often placed over the grafted material to protect the newly growing bone. 2. An appropriate bone grafting material (eg. Bio-Oss®) is carefully placed into the extraction socket. 4. Sutures placed into the gum allow proper healing of the surrounding soft tissue.
 using a biocompatible membrane and an autogenous bone")
GBR Case Guided bone regeneration (GBR) using a biocompatible membrane and an autogenous bone graft mixed with deproteinized bovine bone mineral (Bio -Oss®). Figure 1: Careful flap reflection reveals a narrow ridge (3 -4 mm wide), preventing implant placement at this time. Figure 2: Seven months after the augmentation procedure, there is approximately 8 mm of ridge width available for implant placement. Figure 3: A wide-diameter (5 mm wide x 10 mm long) implant was placed.

FACTORS INFLUENCING REGENERATION Patient factors: Smoking Stress Diabetes mellitus Other systemic conditions Presence of deep multiple pockets

Local factors: Furcal anatomy Thickness of gingival tissue Surgical factors: Infection control, Bone replacement grafts combined with barriers or GTR alone, Type of barrier and surgical technique

Postoperative factors: Plaque control Membrane exposure Membrane retrieval Regular supportive periodontal care program

REFERENCES: Clinical Periodontology & Implant Dentistry by Jan Linde – 3 rd edition Clinical Periodontology by Carranza – 10 th edition Internet Sources: Jcdp. com Osteohealth. com Advancedperiodontics. com Ridental. com Periodont. com Scielo. br

- Slides: 36