Enteric fever Typhoid and paratyphoid fever Is a
 Is a clinical syndrome characterized")











")
 and tender – Widal")





 – Perforation (laparoscopy) Treatment")



- Slides: 25
. Enteric. fever ( Typhoid and paratyphoid fever ) Is a clinical syndrome characterized by constitutional and gastrointestinal symptoms and by headache. Etiologic agents of enteric fever • —S. Typhi and S. Paratyphi and have no known hosts other than humans
Mode of transmission : -The disease is transmitted by faeco - oral route or urine – oral routes – either directly through hands soiled with faeces or urine of cases or carriers or indirectly by ingestion of contaminated water, milk, food, or through flies. Contaminated ice, ice-creams, and milk products are a rich source of infection.
Age group : – Occurs at any age but it is considered to be a disease mainly of children and young adults. – In endemic areas, the highest attack rate occurs in children aged 8 -19 years.
Cont … Gender and race : – commonly seen in males than in females. Occupation : – Certain categories of persons handling the infective material and live cultures of S. typhi are at increased risk of acquiring infection. Socio-economic factors : – It is a disease of poverty as it is often associated with inadequate sanitation facilities and unsafe water supplies.
Cont. . Environmental factors : – peak incidence of typhoid fever is reported during July - September. This period coincides with the rainy season and a substantial increase in fly population. Social factors : – pollution of drinking water supplies, open air defecation, and urination, low standards of food and personal hygiene, and health ignorance.
Cont. . Nutritional status : – Malnutrition may enhance the susceptibility to typhoid fever by altering the intestinal flora or other host defences. Incubation period : – 10 -14 days Reservoir of infection : – Man is the only known reservoir of infection - cases or carriers. Period of communicability: – A case is infectious as long as the bacilli appear in stool or urine.
Cont. . – Carriers : - Temporary or Chronic. Temporary carriers : - usually excrete bacilli up to 6 -8 weeks. – By the end of one year, 3 -4 per cent of cases continue to excrete typhoid bacilli. Chronic carriers: -Persons who excrete the bacilli for more than a year after a clinical attack are called
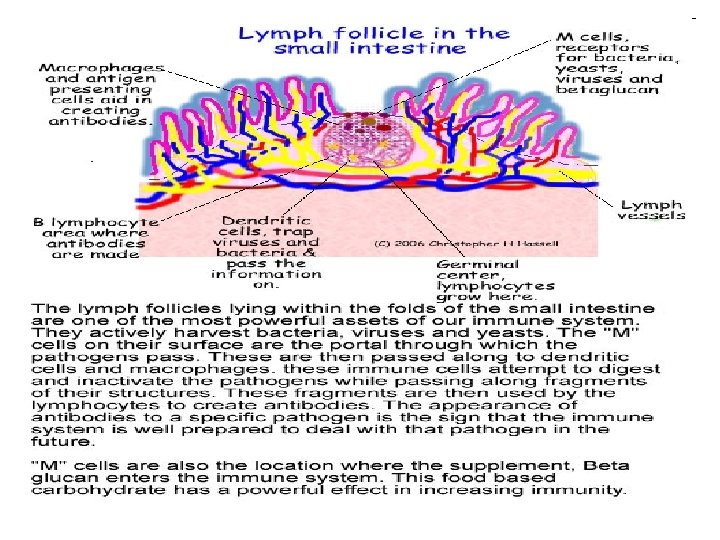
Pathogenesis – Ingestion ------penetration through the intestinal mucosa to the lymphoid tissue of the ileum -------proliferation of the bacteria----macrophages engulf the bacteria -------circulation ( via thoracic duct )-------primary bacteremia ------invasion of blood stream ( onset of fever )-----carried to liver , spleen , marrow where further multiplication occurs ------- secondary bacteremia ( release of large no. of bacteria from reticuloendothelial system----clinical diseases
Cont … • Peyer`s patch : – are the most important organ to get infiltrated with chronic inflammatory cells – Sites for antibody production – Differentiate the ileum from the duodenum and jejunum At the end of 2 nd weeks : – Intestinal and mesenteric lymphnodes : swollen – Liver and spleen : congested and enlarged
Clinical features • Typhoid fever is characterized : – high fever 40 °C (104 °F), profuse sweating, gastroenteritis, and non-bloody diarrhea. – Less commonly a rash of flat, rose-colored spots • Classically, the course of untreated typhoid fever is divided into four individual stages, each lasting approximately one week.
In the first week : There is a slowly rising temperature with relative bradycardia, malaise, headache and cough. – Epistaxis and abdominal pain. – Leukopenia, – Eosinopenia and relative lymphocytosis, – Blood cultures are positive for Salmonella Typhi or Paratyphi.
Cont. . In the second week : – High fever 40 °C (104 °F) and bradycardia – Dicrotic pulse wave. – Delirium is frequent. This delirium gives to typhoid the nickname of "nervous fever". – Rose spots appear on the lower chest and abdomen in around 1/3 patients. – Abdomen is distended and painful in the right lower quadrant
Cont… – Constipation – Spleen and liver are enlarged (hepatosplenomegaly) and tender – Widal reaction is strongly positive with anti. O and anti. H antibodies.
Rose spots
Cont. . • In the third week of typhoid fever a number of complications can occur: – Intestinal hemorrhage due to bleeding in congested Peyer's patches; this can be very serious but is usually non-fatal. – Intestinal perforation in distal ileum; this is a very serious complication and is frequently fatal. – Stool culture ---- positive
Cont. . In the fourth week : – Fever is still very high and oscillates very little over 24 hours. – Dehydration – Delirious (typhoid state) – Urine culture ------ positive
Diagnosis • 15– 25% of cases, leukopenia and neutropenia are detectable. (Leukocytosis is more common among children, during the first 10 days ) • Isolation of S. Typhi or S. Paratyphi from blood, bone marrow, other sterile sites, rose spots, stool, or urine. • Bone marrow culture remains highly (90%) sensitive despite 5 days of antibiotic therapy • Widal test for “Antigen – antibody ’’ • Remember “B A S U”
Treatment General: Supportive care includes : – Maintenance of adequate hydration. – Antipyretics. – Appropriate nutrition. Specific: Antimicrobial therapy is the mainstay treatment. Chloramphenicol , Ampicillin , Amoxicillin , ciprofloxacin, Trimethoprim &Sulphamethoxazole , In case of resistance – 3 rd generation cephalosporins ceftriaxone (50 -100 mg/kg/day in single or two divided doses IV for 5 -7 days) Cefixime (1 o-2 o mg/kg/day in 2 divided doses PO for 7 -10 days) • Treatment should be continued for 14 days
Cont… Treatment of complications : – Intestinal hemorrhage (blood transfusion) – Perforation (laparoscopy) Treatment of carriers : Ceftriaxone IV or ciprofloxacin IV in divided dose for 4 – 6 weeks.
Control Prevention and control Control of reservoir – – – Early diagnosis and notification Isolation- till three culture negative stool/urine Treatment Disinfection of urine/stool Surgery- chronic carrier Health education Control of sanitation – Water supply, basic sanitation, food hygiene, etc. Immunisation – Killed vaccine (anit-typhoid vaccine) – Live oral vaccine.
Specific protection THREE TYPES OF VACCINES 1. Whole cell salmonella typhi vaccine 2. Vi polysaccharide vaccine 3. Oral live attenuated Ty 21 a typhoid vaccine
Complications • • Orodental : Poor orodental hygiene, Parotitis Chest : Bronchitis, Pneumonia, Pulmonary infarct Heart : Myocarditis Liver , Gall bladder : Fatty liver , Hepatitis, Liver Abscess, Cholecystitis, Cholangitis, Pancreatitis. Gastrointestinal : Diarrhoea, Perforation of intestines, Peritonitis & hemorrhage from gut. Neurological : Encephalitis, Encephalopathy, Transverse myelitis, Meningitis, Peripheral neuritis, Aphasia, Cerebral vein thrombosis. Musculoskeletal : Chronic osteomyelitis, Suppurative arthritis, Polymyositis. Miscellaneous : Alopecia , Uveitis