DRUGS USED IN PARKINSONS DISEASE Dr Madushani Silva
 North Colombo Teaching Hospital –")
 is a degenerative disorder of the central")





 �Slowing & poverty of movement is the most disabling feature of")
 & poor asymmetrical")
 �Sensory is normal �Anxiety")






 �Levodopa+benserazide: Co-beneldopa e. g.")






 §Orphenadrine §Procyclidine • Block Ach receptors in the CNS.")




- Slides: 31
DRUGS USED IN PARKINSON’S DISEASE Dr. Madushani Silva (MBBS) North Colombo Teaching Hospital – Ragama
What is Parkinson’s disease �Parkinson's disease (PD) is a degenerative disorder of the central nervous system with motor system disorders, which are the result of the loss of dopamine -producing brain cells �Usually affects people over the age of 50
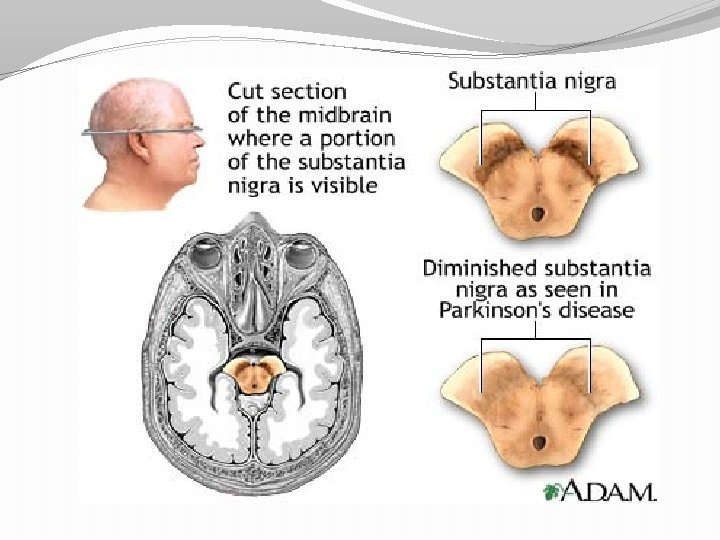
Idiopathic Parkinson’s disease �Pathology �Progressive degeneration of cells within the substantia nigra �Loss of dopaminergic cells in the substantia nigra causes a reduction in dopamine in the striatum �Degeneration also occurs in the other basal ganglia nuclei
Aetiology �Cause is unknown
Clinical features �Classical triad of tremor, rigidity & bradykinesia, in association with changes in posture & gait �An important characteristic feature of Parkinson’s disease is the striking asymmetry of the clinical signs �initially more prominent on one side �Symptoms develops slowly, over months or several years �Most common initial symptoms are tremor & slowness
�Tremor �Characteristic coarse resting tremor usually decreased with action of tremulous limb & increased with emotion & distraction (walking or using the contralateral limbs) �Tremor disappears during sleep �Often “pill-rolling nature” - thumb moves rhythmically backwards & forwards on the palmar surface of the fingers �Resting tremor can affect the any part of the body including chin, tongue & feet
�Rigidity �Lead pipe rigidity – stiffness of the limbs, which can be felt throughout the range of movement & equally in the flexors & the extensors �When stiffness occurs with the tremor, smooth ‘lead pipe’ rigidity is broken up in to a jerky resistance to passive movement known as cogwheeling or cogging �Rigidity is usually asymmetrical in the limbs
�Bradykinesia (akinesia, hypokinesia) �Slowing & poverty of movement is the most disabling feature of the Parkinson’s disease �There is difficulty in initiating & terminating the movements �Rapid fine finger movements (piano-playing) become indistinct �Bradykinesia & hypokinesia also affects to muscles of facial expression, so facial immobility gives masklike semblance of depression (hypomimia) �Frequency of spontaneous blinking is reduced
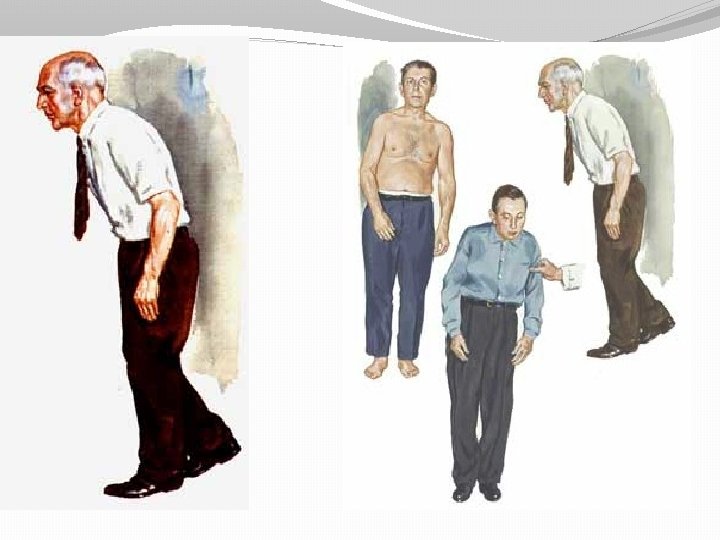
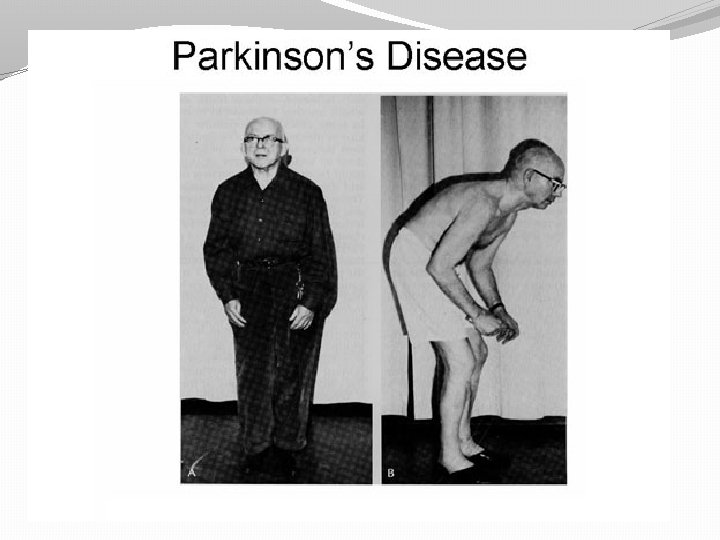
�Postural changes �Posture is characteristically shuffling, forward flexed, festinant gait (hurrying) & poor asymmetrical arm swing �Falls are common later in the disease �When pt tries to turn either when walking or lying (in bed), there are greater difficulty �Speech is altered, initially monotonus but progress to tremulous slurring dysarthria due to a combination of bradykinesia, rigidity & tremor
�Other features �Handwriting reduces in size & become spidery (micrographia) �Sensory is normal �Anxiety & depression are common �Cognitive function is preserved in the early stages but dementia occur at later. �Heartburn, dysphagia, constipation & weight loss �Urinary difficulties are common �Reflexes are active and energitic. �Skin is greasy & sweating excessive
Micrographia The main problem in this disease is Mask-like expressionless face Flexed posture Pill-rolling tremor of the hand Stiff, shuffling posture
Main categories �Dopaminergic drugs used in parkinsonism �Antimuscarinic drugs used in parkinsonism
Principles of Drug Treatment �Each patient with PD may present with a different pattern of the disease. Therefore the management should be individually decided. �Drug treatment should be started only when it is decided necessary in each individual case. �Parkinson’s Disease is relatively easily controlled in the first few years.
Principles of Drug Treatment �About 50% of patients experience significant complications of treatment after 5 years. �the gain of controlling symptoms should be compared with the adverse effects of long-term drug treatment. �The mainstay of antiparkinsonian therapy is restoring Dopaminergic /Cholinergic balance.
�Dopaminergic /Cholinergic balance is achieved by: Ø Enhancing dopaminergic activity by drugs that: v replace neuronal Dopamine: Levodopa v act as Dopamine agonists: Bromocriptine v prolong the action of Dopamine by selective inhibition of its metabolism: MOA-B Inhibitor- Selegiline v release Dopamine from stores and inhibit re-uptake: Amantadine
ØReduction of Cholinergic activity by anticholinergic drugs: drugs acting as antagonists on the muscarinic cholinergic receptors (antimuscarinic drugs): Benzhexol �
Drugs Enhancing Dopaminergic Activity Dopamine replacement: Levodopa (Levodopa+peripheral dopadecraboxylase inhibitor) �Levodopa+benserazide: Co-beneldopa e. g. Co-beneldopa 25/100 – benserazide 25 mg + Levodopa 100 mg �Levodopa+carbidopa: Co-careldopa e. g. Co-careldopa 12. 5/50 – carbidopa 12. 5 + Levodopa 50 mg § Why this combination? * make more levodopa available to cross the BBB: *prevent peripheral side effects by preventing Dopamine formation peripherally: nausea, vomiting, CVS effects.
§ LEVO-DOPA, DOPA= dihydroxyphenylalanine (natural amino acid precursor of dopamine. § Dopamine is not given as it is: o rapidly metabolized in the gut, liver and blood by monoamine oxidase (MAO) and catechol-Omethyltransferase (COMT). o Not lipid soluble enough to cross the BBB § Levodopa is well absorbed in the upper small intestine by active amino acid transport. § Levodopa reaches the CNS by crossing the BBB by a similar active amino acid transport mechanism.
§ less valuable in post - encephalitic parkinsonism, elderly patients and in long standing disease. § Provides biggest improvement in motor symptoms, when compared to other drugs. § Associated with development of dyskinesias after 5 -10 years of its use, sometimes earlier than this. § Abrupt discontinuation of therapy result in relapse.
§ Adverse effects: �Levodopa-induced dyskinesia: involuntary limb jerking, head, lip or tongue movements. Mental changes: depression, dreams, hallucinations, delusions
Increasing Dopaminergic Activity Dopamine agonists Supress prolactin release: inhibit effect on the anterior pituitary. § § § Bromocriptine Pergolide Lisuride Cabergoline Ropinirole Pramipexole
�Less likely to cause dyskinesias, but have less powerful motor effects when compared with levodopa, only about 30% of patients show improvement in motor symptoms. Drugs prolonging the action of Dopamine by selective inhibition of its metabolism Monoamine oxidase -B-inhibitors § Selegiline �Used in early mild cases to delay the use of levodopa or dopamine agonists. Catechol-O-Methyl Transferase Inhibitors (COMTI) § Entacapone �Helps to relieve end of dose deterioration without causing dyskinesia.
Drugs releasing Dopamine: § Amantadine �Is an antiviral drug. �Increase synthesis and release of dopamine. �Inhibit neuronal re-uptake of dopamine. �Has slight antimuscarinic effects. �More effective than antimuscarinic drugs. �Relatively free of side effects. � .
Antimuscarinic Drugs §Benzatropine §Benzhexol (trihexiphenidyl) §Orphenadrine §Procyclidine • Block Ach receptors in the CNS. • no significant action on bradykinesia. • Useful in drug-induced parkinsonism. • Benztropine & Procyclidine available as injections: Rx for acute dystonic reaction. • Side effects: anticholinergic effects.
�Levodopa - release brain dopamine from nerve endings making it more available to activate dopaminergic receptors, Bromocriptine – dopamine receptor agonist
�Antimuscarinic drugs exert their antiparkinsonian action by reducing the effects of the central cholinergic excess that occur as a result of dopamine deficiency
Questions ?
THANK YOU