Dr Swarnalatha Devi MD Professor of Medicine MITRA










. This is due to")












. n Open")




- Slides: 29
Dr. Swarnalatha Devi MD Professor of Medicine
MITRA VALVULAR DISEASE
MITRAL STENOSIS Aetiology and pathophysiology n Mitral stenosis is almost always rheumatic in origin, although in the elderly it can be caused by heavy calcification of the mitral valve apparatus. n n There is also a rare from of congenital mitral stenosis.
AETIOLOGY n Rheumatic heart disease. n Congenital—parachute mitral valve. n Hunter”, hurler” syndrome. n Drugs---methysergide. n Carcinoid syndrome.
PATHO PHYSIOLOGY n In rheumatic mitral stenosis, the mitral valve orifice is slowly diminished by progressive fibrosis, calcification of the valve leaflets, and fusion of the cusps and subvalvular apparatus. n The flow of blood from left atrium to left ventricle is restricted and left atrial pressure rises, leading to pulmonary venous congestion and breathlessness. n There is dilatation and hypertrophy of the left atrium, and left ventricular filling becomes more dependent on left atrial contraction.
PATHOPHYSIOLOGY Any increase in heart rate shortens diastole when the mitral valve has to open it produces further rise in left atrial pressure; n Situations that demand an increase in cardiac output will also increase left atrial pressure. n n Exercise and pregnancy are therefore poorly tolerated.
n The mitral valve orifice is 4 -5 cm 2 in diastole and may be reduced to 1 cm 2 or less in severe mitral stenosis. Patients usually remain asymptomatic until the stenosis is approximately 2 cm 2 or less. n At first, symptoms may occur only on exercise, in severe stenosis, left atrial pressure is permanently elevated so breathlessness occurs even at rest due to. Chronic pulmonary venous congestion. n Low cardiac output may cause fatigue. n
n Pulmonary hypertension may lead to right ventricular hypertrophy and dilatation, tricuspid regurgitation and right heart failure. n Less than 20% of patients remain in sinus rhythm; many of these have a small fibrotic left atrium and severe pulmonary hypertension. n All patients with mitral stenosis, and particularly those with atrial fibrillation, are at risk from left atrial thrombosis and systemic thromboembolism. .
SYMPTOMS n Dyspnoea. n Palpitations. n Fatigue. n Hemoptysis. n Recurrent bronchitis.
CLINICAL EXAMINATION n MITRAL FACIES. n SMALL VOLUME PULSE. n LEFT PARASTERNAL HEAVE. n TAPPING APICAL IMPULSE (PALPABLE S 1)
n Loud S 1 , opening snap, (in pliable valve). This is due to diastolic buckling of anterior mitral or tricuspid leaflet due to elevated left or right atrial pressure. n A low pitched , rough , rumbling mid diastolic murmur with pre systolic accentuation best heard over apex, with bell of stethoscope in left lateral position, in expiration. n ESM over pulmonary area if there is PAH. Pan
Mitral Stenosis: Physical Exam S 1 n n S 2 OS S 1 First heart sound (S 1) is accentuated and snapping Opening snap (OS) after aortic valve closure Low pitch diastolic rumble at the apex Pre-systolic accentuation (esp. if in sinus © Continuing Medical Implementation …. . . bridging the care gap rhythm)
INVESTIGATIONS ECG—”P” MITRALE AND RIGHT VENTRICULAR HYPERTROPHY. n ATIAL FIBRILLATION ---ABSENT P WAVES , VARYING R-R INTERVALS. n X—RAY CHEST—LEFT ATRIAL ENLARGEMENT n STRAIGHTENING OF LEFT BORDER n KERLY A, B LINES n R A O WITH BARIUM SWALLOWCOMPRESSION BY LEFT ATRIUM n
A 75 year old woman with loud first heart sound and mid-diastolic murmer © Continuing Medical Implementation …. . . bridging the care gap
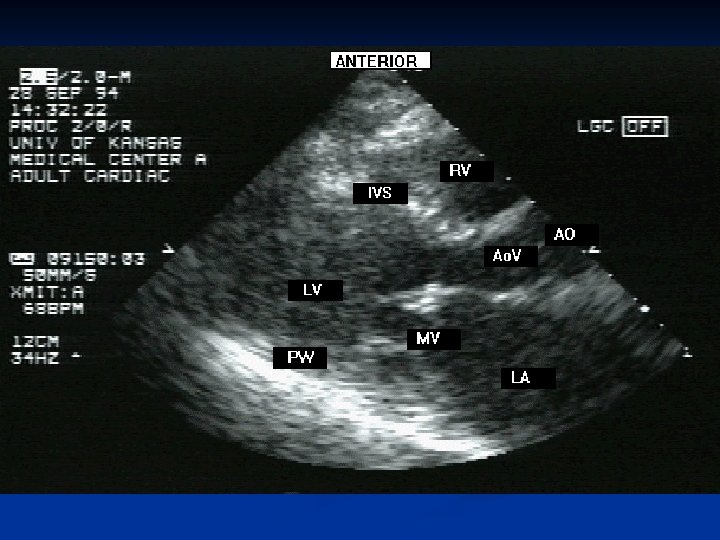
n ECHO CARDIOGRAM—THICKENED , IMMOBILE CUSPS, REDUCED RATE OF DIASTOLIC FILLING. REDUCED VALVE AREA. CARDIAC CATHETERISATION— PRESSURE GRADIENT BETWEEN LA AND LV n
Mitral Stenosis
SEVERITY n ACCORDING TO VALVE AREA---- n -4 -6 cm 2 ------NORMAL n > 2. 5 cm 2 ------NO SYMPTOMS n 1. 5— 2. 5 cm 2 ---MILD n n 1 -1. 5 cm 2 ---MODERATE- -DYSPNOEA ON EXERTION PND +P. EDEMA <1 cm 2 ---SEVERE /CRITICAL -ORTHOPNEA –CLASS 1 V
ACCORDING TO A 2—OS INTERVAL n IN SEVERE MS---- THIS PERIOD IS SHORTENED. — 0. 05 -0. 07 SEC n MILD MS— 0. 10 -0. 12 SEC n ACCORDING TO PRESSURE GRADIENT ACROSS MITRAL VALVE— n MILD-<5 mm Hg n MODERATE— 5— 15 mm Hg n SEVERE-->15 mm Hg n DURATION OF DIASTOLIC MURMUR IS DIRECTLY PROPORTIONAL TO THE SEVERITY n
COMPLICATIONS n HEMOPTYSIS--- n Due to pulmonary apoplexy. n Acute LVF—pulmonary edema. n Pulmonary congestion. n Recurrent bronchitis. n Pulmonary infarction.
n ATRIAL FIBRILLATION-- n 2/3 will have AF n Pulse is irregularly irregular n No a waves in JVP n Intensity of S 1 is variable n AF precipitates---CCF, thrombo embolic phenomenon
n Infective endocarditis. n Pressure symptoms----ortners syndrome---compression of recurrent laryngeal nerve by left atrium. n Left bronchus--bronchiectasis.
DIFFERENTIAL DIAGNOSIS n Left atrial myxoma. n Cortriatritum. n Ball valve thrombus of left atrium. n Flow murmurs of VSD, ASD, PDA. n Carey-coombs murmur.
Medical Management n Anti failure measures. n Anticoagulation in n Rheumatic fever prophylaxis. n Infective endocarditis atrial fibrillation. prophylaxis.
SURGICAL TREATMENT n Closed mitral valvotomy/commissurotomy— (with out cardio pulmonary by pass). n Open mitral valvotomy/commissurotomy (with aid of cardio pulmonary by pass). n Per cutaneous balloon valvuloplasty. n Mitral valve replacement.
n Closed mitral valvotomy—in pliable valve and , no mitral regurtitation n Open mitral valvotomy---in this valve, sub valvular. C hordae tendinae are loosened, calcific deposits removed Thrombi if present are removed.
n Percutaneous balloon valvuloplasty---in pregnant women, Severe extracardiac disease. Criterian -Significant symptoms n Isolated MS. n No mitral regurgitation. n Mobile, non calcified valve. Normal sub valvular apparatus n No thrombus in left atrium
VALVE REPLACEMENT---n Associated MITRAL REGURGITATION n Valve rigid, and calcified. n Mechanical prosthesis— n Caged ball valve(starr-edward prosthesis). n TILTING DISK valves(st jude. Bjork-shiely
THANK YOU