Primary Ovarian Insufficiency By Dr Mitra Kazemi Fellowship

Primary Ovarian Insufficiency By: Dr Mitra Kazemi Fellowship Of endocrinology. Shahid Beheshti University of medical sciences
 l Diagnosis (…and Role of AMH) l Clinical manifestations(short")
Agenda Etiology of POF(Autoimmune ophoritis) l Diagnosis (…and Role of AMH) l Clinical manifestations(short term sequela, effects on CVD, osteoporosis, Breast and endometrial cancer, cognition, , ) l Hormon replacement therapy (difference between HRT and COCP, effects of HRTon cognition, Breast cancer, role of testesterone…) l Outcome l

Up to date 2017

Autoimmune Ophoritis l Autoimmune oophoritis may occur as part of type I and type II syndromes of polyglandular autoimmune failure, l It has been reported to occur in approximately 5% of cases of POI , Post Reproductive Health 2017, Vol. 23(1) 22– 35

l The majority of cases with autoimmune POI have autoimmunity involving other organs, the commonest being adrenal autoimmunity, estimated to occur in approximately 60%– 80% of cases with autoimmune POI. l Thyroid autoimmunity is estimated to occur in approximately a fifth of cases with autoimmune POI. Post Reproductive Health 2017, Vol. 23(1) 22– 35

But What Will Happen to LH and FSH in Autoimmune Ophoritis?

l Methods: We have determined the serum concentrations of total inhibin and inhibin B by sensitive ELISAs in: 22 women with autoimmune POI, 71 women with non-autoimmune idiopathic POI, 77 postmenopausal women, and 90 healthy, fertile women.
: 1263 -9. doi: 10. 1210/jc. 2007 -1675.")
J Clin Endocrinol Metab. 2008 Apr; 93(4): 1263 -9. doi: 10. 1210/jc. 2007 -1675. Epub 2 008 Jan 22.
: 266 women with 46, XX spontaneous premature ovarian failure. l Intervention(s): Ovarian biopsy")
Patient(s): 266 women with 46, XX spontaneous premature ovarian failure. l Intervention(s): Ovarian biopsy in 10 women. As stipulated by the protocol, to qualify for ovarian biopsy women had to have had either a coexisting autoimmune disease, a positive test for an organ specific autoantibody, or a first degree relative with an autoimmune disease l Fertility and Sterility Vol. 84, No. 4, October 2005

Fertility and Sterility Vol. 84, No. 4, October 2005

l Conclusion: l In women who present with 46, XX spontaneous premature ovarian failure as their primary concern there is a clear association between serum adrenal cortex autoantibodies and the presence of histologically confirmed autoimmune oophoritis. Fertility and Sterility Vol. 84, No. 4, October 2005

l What is the role of Autoantodies in the Dx of POF?

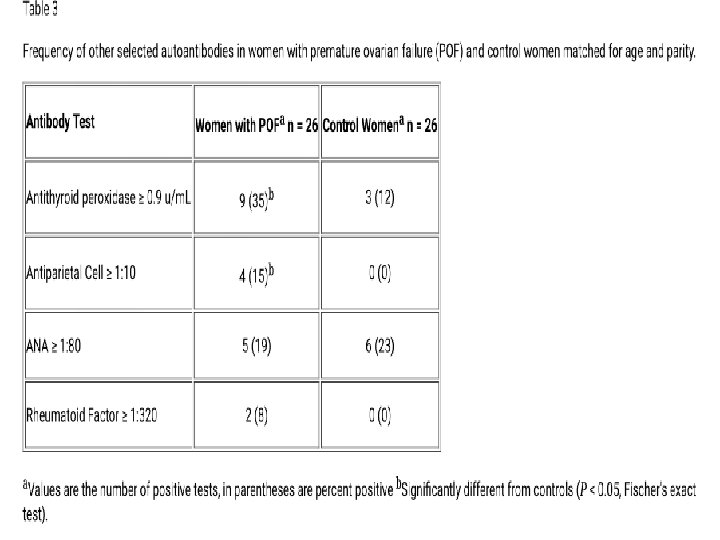
l The test was performed in a blinded manner in 26 young women with 46, XX spontaneous premature ovarian failure, in 26 control women with regular menstrual cycles (matched for age, race, and parity) and 26 control men (matched for age and race). We also compared the frequency of other autoantibodies associated with ovarian autoimmunity. BMC Women's Health 20033: 2
 of normal control women had ovarian antibodies using the")
l Unexpectedly, however, nearly 1/3(31%) of normal control women had ovarian antibodies using the commercially available test. l 1/2 of young women with POF were found to have ovarian antibodies (P = 0. 26). l None of 26 men were found to have ovarian antibodies (P < 0. 001). BMC Women's Health 20033: 2
 l Diagnosis (…and Role of AMH) l Clinical manifestations(short")
Agenda Etiology of POF(Autoimmune ophoritis) l Diagnosis (…and Role of AMH) l Clinical manifestations(short term sequela, effects on CVD, osteoporosis, Breast and endometrial cancer, cognition, , ) l Hormon replacement therapy (difference between HRT and COCP, role of Testostrone…) l Outcome l

Diagnosis of POI: l The diagnosis of POI is based on a combination of oligomenorrhoea/ amenorrhoea of more than 4 months’ duration associated with elevated gonadotropins (FSH >40 IU/l) on at least two occasions measured 4 -6 weeks apart in women under the age of 40. l

What is the role of AMH in the diagnosis of POI?

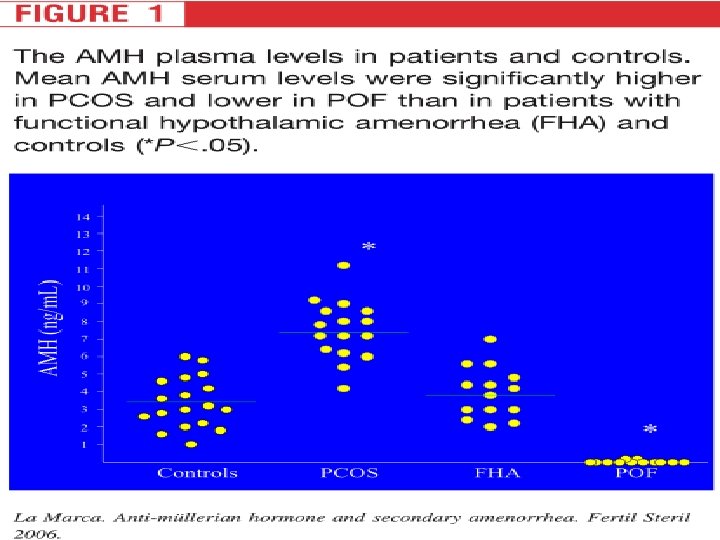
Methods: The study design included four groups of women (3 groups of women affected by secondary amenorrhea and 1 control group): l group 1 consisted of patients with hypergonadotropic amenorrhea(POF) (n: 12; age, 23– 35 years); l group 2 consisted of patients with FHA (n 14; age range, 17– 31 years) Fertility and Sterility Vol. 85, No. 5, May 2006
 (n 16; age range,")
l group 3 consisted of patients with normo-gonadotropic amenorrhea (PCOS) (n 16; age range, 18– 29 years); l group 4 consisted of healthy control women with regular menstrual cycles (n 18; age range, 20– 37 years). Fertility and Sterility Vol. 85, No. 5, May 2006

However, very low or undetectable levels of AMH, while suggestive of diminished ovarian reserve, are not sufficient for the diagnosis of POI especially in the presence of regular menstrual cycles. l AMH should therefore not be routinely used to diagnose POI but may have a role when the diagnosis of POI is inconclusive. l
 l Diagnosis (…and Role of AMH) l Clinical manifestations(short")
Agenda Etiology of POF(Autoimmune ophoritis) l Diagnosis (…and Role of AMH) l Clinical manifestations(short term sequela, effects on CVD, osteoporosis, Breast and endometrial cancer, cognition, , ) l Hormon replacement therapy (difference between HRT and COCP, role of testesterone…) l Outcome l
 are the commonest menopausal")
Short-term Sequelae l Vasomotor symptoms (hot flushes and night sweats) are the commonest menopausal symptoms reported in women with POI. l In addition, women with POI may experience insomnia, joint pain, labile mood, low energy, low libido as well as impaired memory and concentration.

l Symptoms related to urogenital atrophy have been reported in approximately 40%– 50% of women with POI. l These may present as vaginal dryness, dyspareunia, urinary frequency and urinary incontinence. l In addition, it has been reported that approximately 12%– 14% of women with POI do not experience menopausal symptoms.

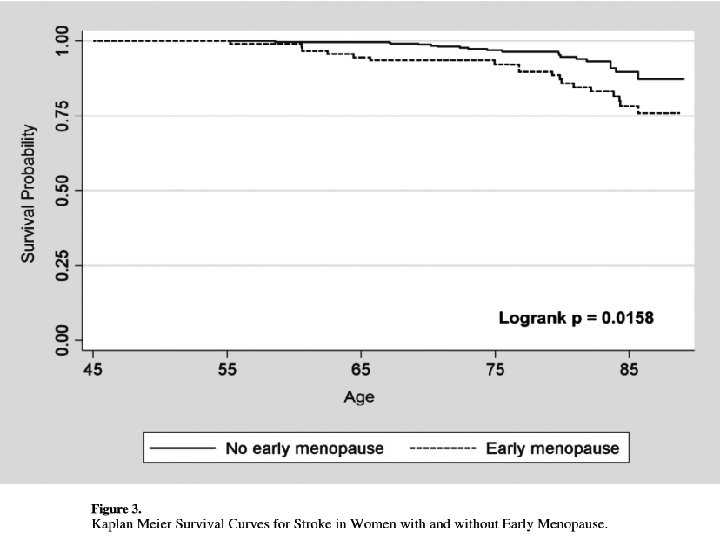
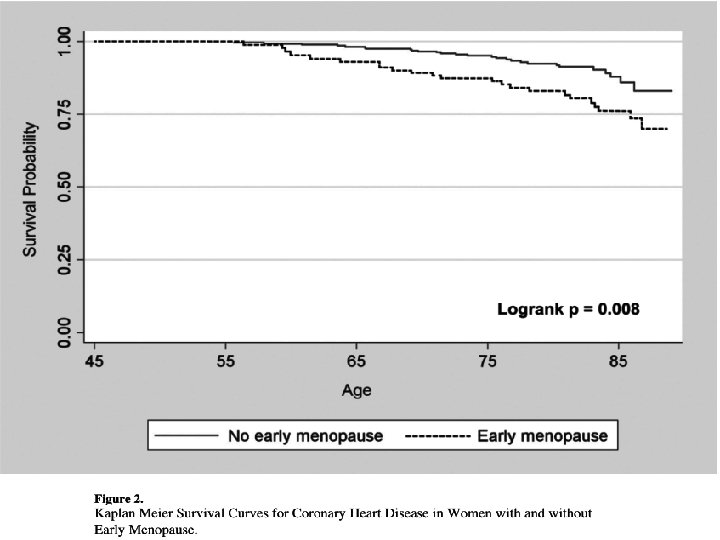
Methods l Methods: The study population came from the Multi- Ethnic Study of Atherosclerosis, a longitudinal, ethnically diverse cohort study of US men and women aged 45 - 84 years enrolled in 2000– 2002 and followed up until 2008.

l The association between a personal history of early menopause and future coronary heart disease and stroke was assessed in 2509 women (ages 45– 84, 987 White, 331 Chinese, 641 Black, 550 Hispanic) from the Multi-Ethnic Study Atherosclerosis, who were free of cardiovascular disease at baseline.

l Methods: A total of 390 white north European women aged 48 years icluded at the start of the study. Women were divided into early menopause (occurring before age 47 years) and late menopause (occurring at age 47 years or later). At age 77, forearm BMD and proximal femur and lumbar spine BMD were measured. Mortality rate and the incidence of fractures were registered up until age 82.

l Results: l Women with early menopause had a risk ratio of 1. 83(1. 22 -2. 74) for osteoporosis at age 77,
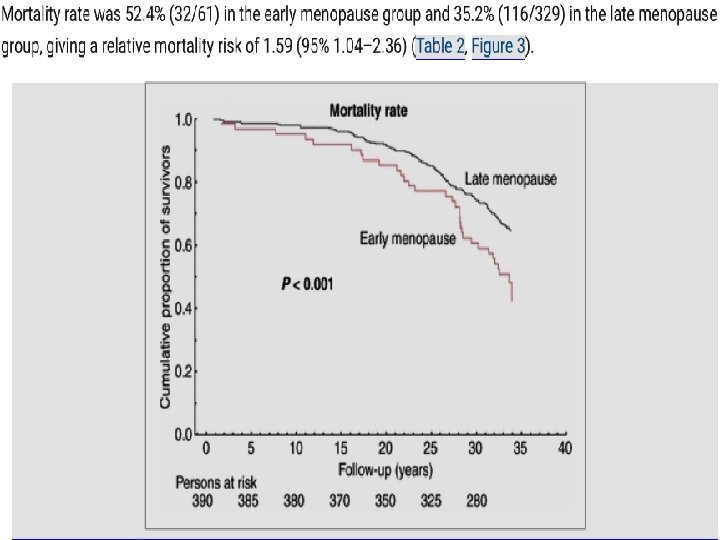

In the early menopause group, the fracture incidence per 10 person-years was 19. 45 compared with 11. 60 in the late menopause group, giving a risk ratio of 1. 68 (95% CI 1. 05– 2. 57) for sustaining a fragility fracture l

Methods: We identified 1, 003 cases of POF among 36, 402 postmenopausal women who participated in the Shanghai Women’s Health Study, a population-based cohort study. March 2014 | Volume 9 | Issue 3 | e 89597

Results After adjustment for potential confounding factors, we found that POF increased the risk of total mortality (HR (95%CIs): 1. 29 (1. 08– 1. 54) cancer specific mortality (HR (95%CIs): 1. 38 (1. 05– 1. 81) March 2014 | Volume 9 | Issue 3 | e 89597

l POF was also associated with : l high prevalence of autoimmune disease (OR (95%CI): 1. 56 (1. 04– 2. 35)) l decreased incidence of breast cancer (OR (95%CI): 0. 59(0. 38– 0. 91)). l Similar results were observed when hormone replacement therapy users were excluded from the analysis March 2014 | Volume 9 | Issue 3 | e 89597

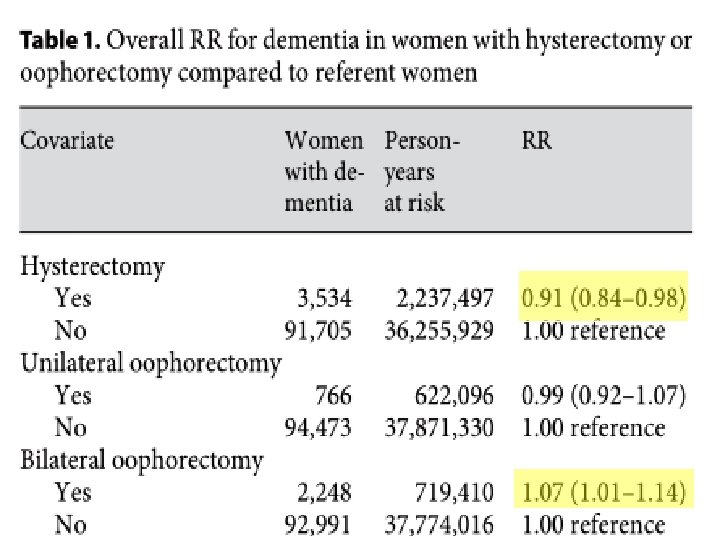
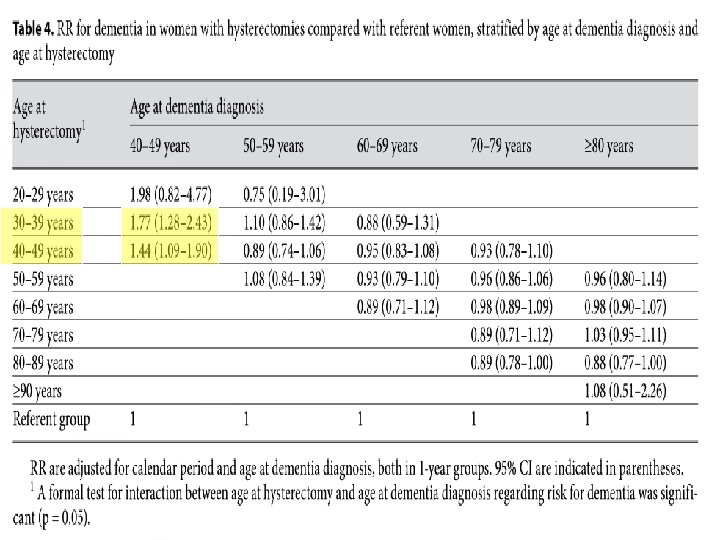
Methods All female Danish residents born before 1966, alive on their 40 th birthday and without a dementia diagnosis prior to 1977 (n = 2, 313, 388) were followed from January 1, 1977, or the age of 40, whichever came later, until dementia diagnosis or December 31, 2006 whichever came first. (RR) for developing dementia in women with hysterectomy/oophorectomy compared to referent women were calculated.

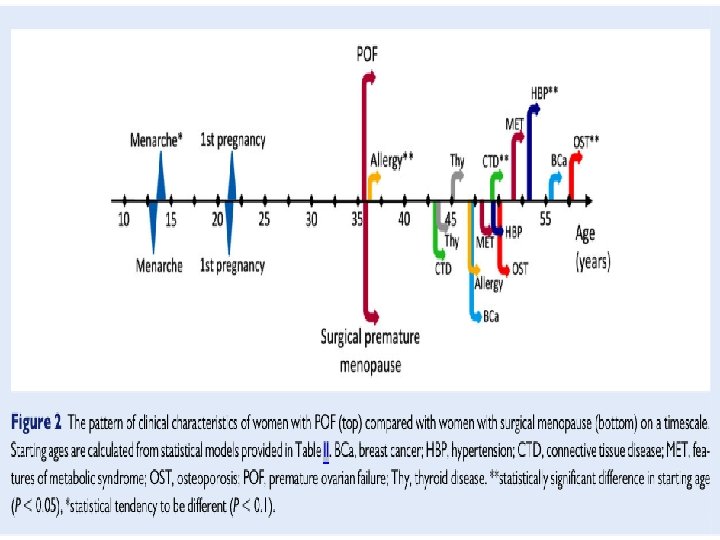
Methods: This study included 34 041 women from the Estonian Genome Center registered between 2003 and 2013. l Spontaneous POF was selected retrospectively by excluding other causes for premature menopause under the age of 40 (310) and women with surgically induced POF participated as a reference group (242). l
 l Diagnosis (…and Role of AMH) l Clinical manifestations(short")
Agenda Etiology of POF(Autoimmune ophoritis) l Diagnosis (…and Role of AMH) l Clinical manifestations(short term sequela, effects on CVD, osteoporosis, Breast and endometrial cancer, cognition, , ) l Hormone replacement therapy (difference between HRT and COCP, effects of HRTon cognition, Breast cancer, role of Testostrone…) l Outcome l
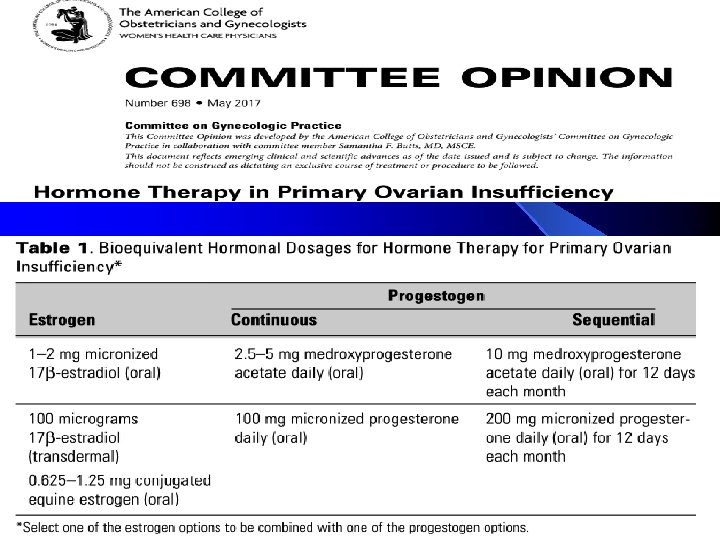

Systemic sex steroid hormone replacement is effective for the management of menopausal symptoms in women with POI and topical estrogen preparations are effective for the management of symptoms related to urogenital atrophy.

It has been reported that approximately 12%– 14% of women with POI do not experience menopausal symptoms. This group, still be advised to have hormone replacement for the prevention of the longterm sequelae of POI including bone and cardiovascular protection.

Is there any difference between HRT and COCP in the Rx of the patients with POF? ?

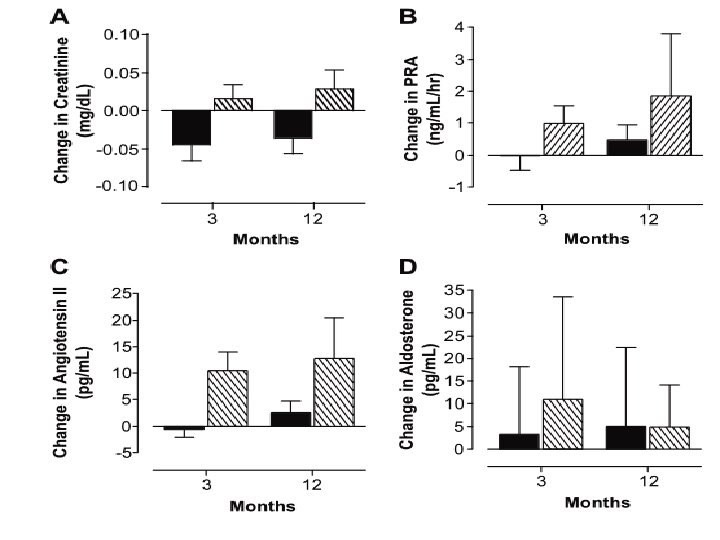
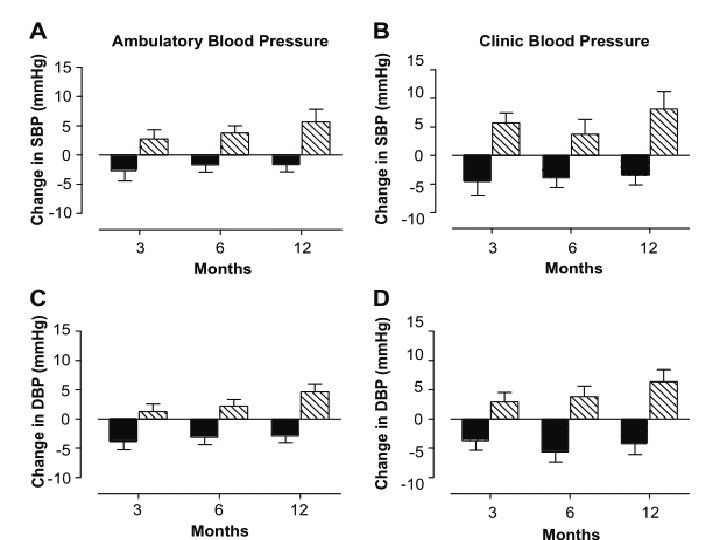
Methods: 42 women with premature ovarian failure attributed to chemotherapy or radiotherapy, idiopathic or surgical treatment, or Turner syndrome were recruited between February 2002 and November 2006(United Kingdom). l At entry, all of the patients were receiving a standard nonphysiological hormone replacement regimen. l Hypertension. 2009; 53: 805 -811 Originally published April 22, 2009

After a 2 -month washout period of no therapy, patients were randomly assigned to receive either the standard regimen (Loestrin 30; ethinylestradiol 30. 0 μg and norethisterone 1. 5 mg daily for weeks 1 to 3, followed by 7 “pill-free” days) or l physiological sex steroid replacement transdermal estradiol 100 μg daily for week 1 and 150 μg for weeks 2 to 4: and (dydrogesterone 10 mg twice daily in weeks 3 to 4). l Hypertension. 2009; 53: 805 -811 Originally published April 22, 2009

l Cardiovascular health assessments were made at the start of the first washout period, at the end of each washout period, and at 3, 6, and 12 months of each treatment period. Hypertension. 2009; 53: 805 -811 Originally published April 22, 2009

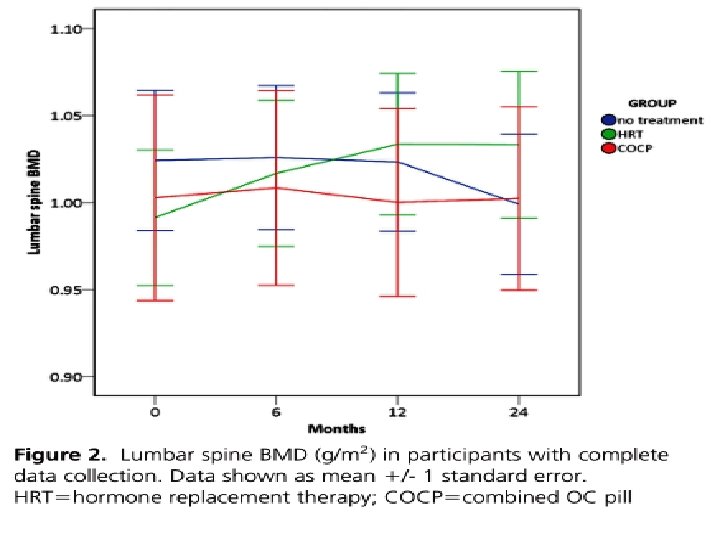
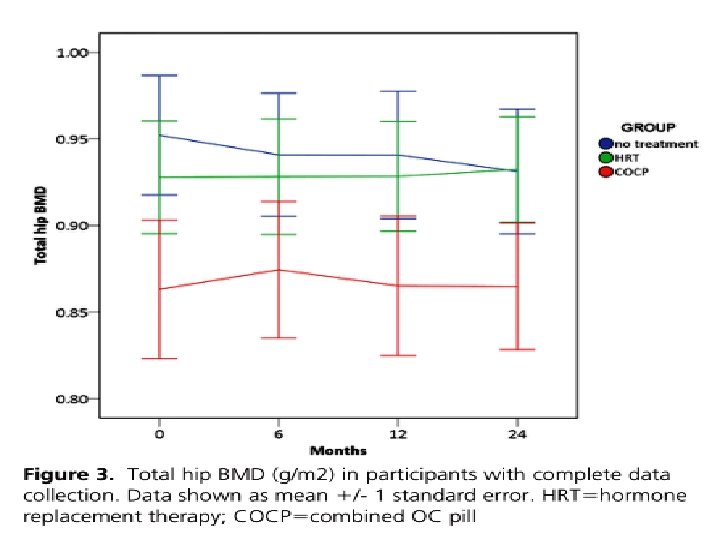
Methods: 59 women with spontaneous POF aged 18– 44 women elected to take treatment and were randomised in a London teaching hospital. l Intervention: Randomisation was to HRT (Nuvelle) or COCP (Microgynon 30). Main outcome measures: l The primary outcome was change in lumbar spine BMD. Changes in total hip and femoral neck BMD and bone turnover markers were also assessed. l doi: 10. 1210/jc. 2015 -4063 J Clin Endocrinol Metab

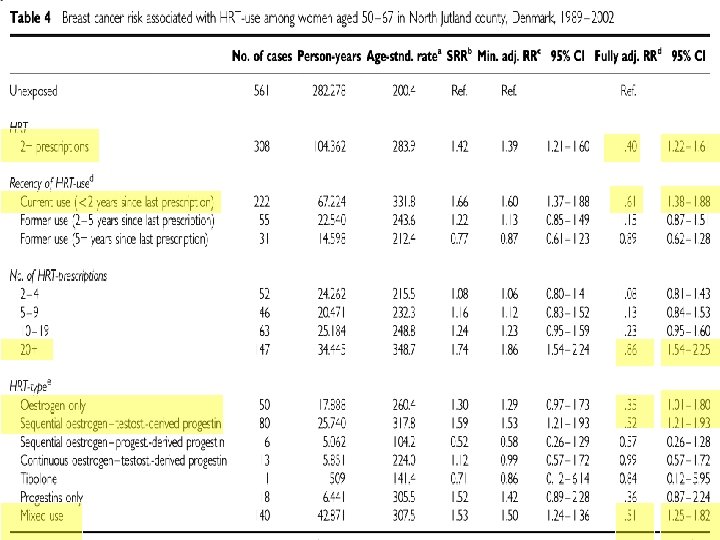
Using longitudinal data from the population-based prescription database of the county of North Jutland, Denmark, and the Danish Cancer Registry, we examined the risk of developing breast cancer in relation to HRT in a cohort of 78, 380 women aged 40– 67 years from 1989 to 2002. A total of 1462 cases of breast cancer were identified during a mean follow-up of 10 years. l

By: Dr Mitra Kazemi Fellowship of endocrinology. Shahid Beheshti University of medical sciences

Unopposed estrogen replacement therapy is an important risk factor for endometrial hyperplasia (10– 50% incidence/year) and cancer (up to a 10 -fold increase in absolute risk) and, therefore, is not recommended. l The addition of progestogen therapy (sequential or continuous doses)to estrogen replacement significantly reduces the risk; l

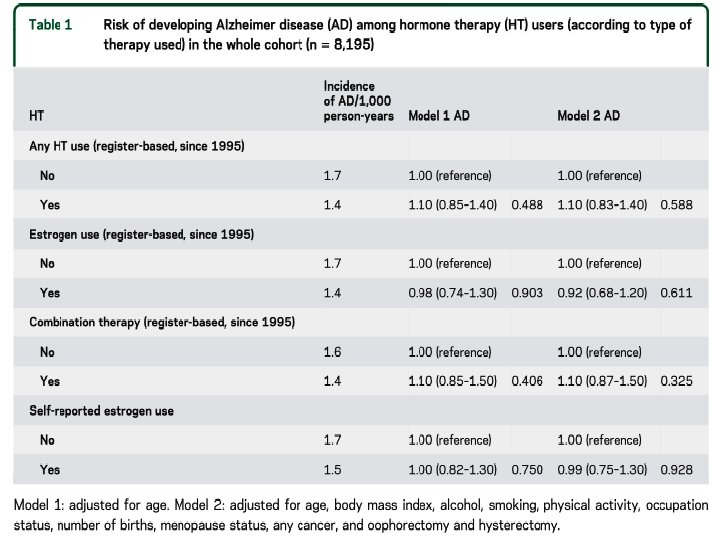
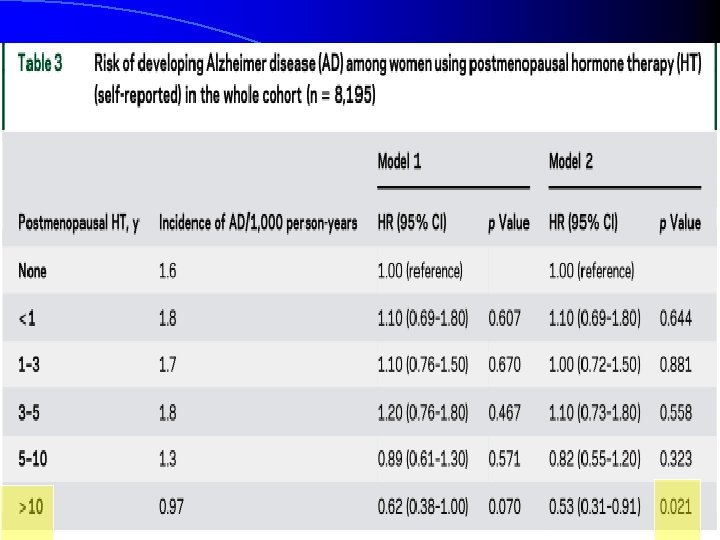
Methods l Methods: Twenty-year follow-up data from the Kuopio Osteoporosis Risk Factor and Prevention study cohort were used. Self-administered questionnaires were sent to all women aged 47– 56 years, residing in Kuopio Province starting in 1989 until 2009, every 5 th year. Register-based information on HT prescriptions was available since 1995. Neurology® 2017; 88: 1062– 1068

What is the role of Testosterone in the Rx of the patients with POI?

Methods: 128 women with 46 XX spontaneous POI participated in a 12 month randomized, placebocontrolled study. l Quality of life, self-esteem, and mood symptoms were evaluated with standardized rating scales and a structured clinical interview. l
.")
Results No differences were found in baseline characteristics including serum hormone levels(P >0. 05). l Baseline mean(SD) CES-D scores were 10. 7(8. 6)(T) and 9. 2(7. 8)(placebo) (P = 0. 35). l After 12 months of treatment, measures of quality of life, self-esteem, and the presence of mood symptoms did not differ between treatment groups. l

l Serum T levels achieved physiologic levels in the T group and were significantly higher compared to placebo (P < 0. 001). l Baseline T levels were not associated with either adverse or beneficial clinical effects.
on BMD. We")
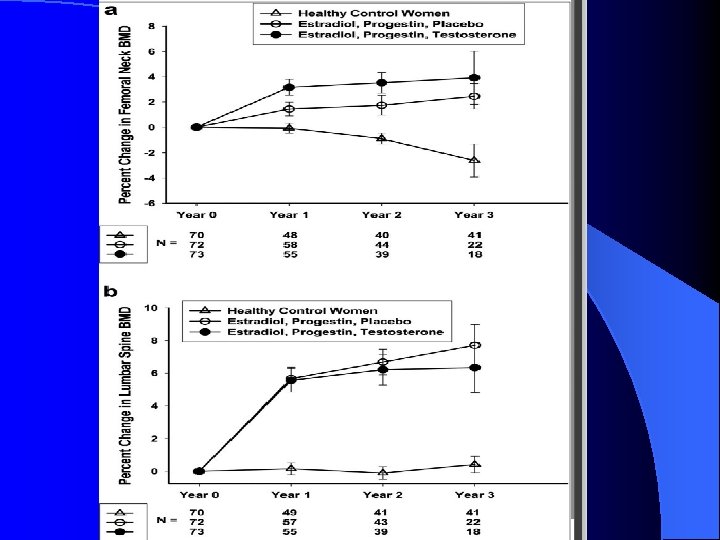
Methods: We compared the effect of estradiol, progestin and T replacement (n=73)on BMD. We also compared findings with a control group of normal women(n=70). l All patients received transdermal estradiol (100 mg/dl)plus oral medroxyprogestrone acetate 10 mg/d for a 3 month period before being randomized in a double blinded fashion to the addition of transdermal T(150 mg/d) or placebo. Change in BMD at the femoral neck and lumbar spine was measured. l
 l Diagnosis (…and Role of AMH) l Clinical manifestations(short")
Agenda Etiology of POF(Autoimmune ophoritis) l Diagnosis (…and Role of AMH) l Clinical manifestations(short term sequela, effects on CVD, osteoporosis, Breast and endometrial cancer, cognition, , ) l Hormon replacement therapy (difference between HRT and COCP, role of Testostrone…) l Outcome l

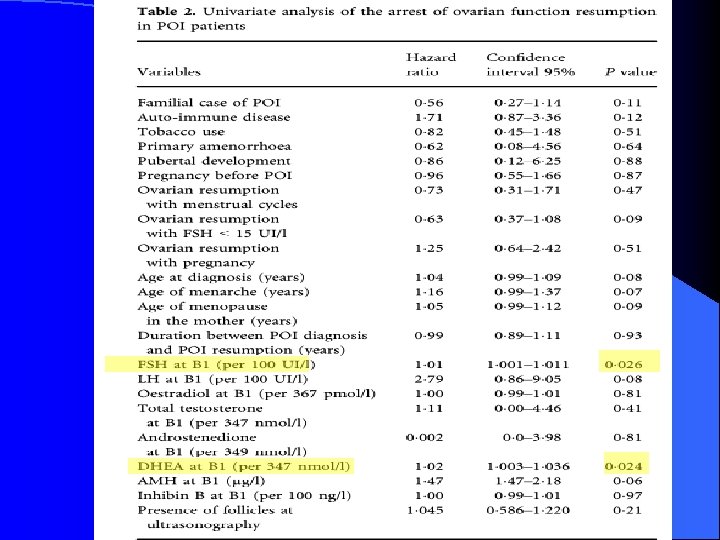
Methods: A cohort of POI patients was set up in our department in 2001. This included idiopathic POI patients referred to the university medical center in Paris since 1997 and included 542 consecutive patients on December 2013. These patients were studied retrospectively before 2001 and thereafter prospectively.

l Cumulative incidence of ovarian function resumption and risk factors arresting this resumption during follow-up were determined in a large cohort of POI women.

l Results: l The cumulative incidence of pregnancy was 3. 5% among the whole cohort and 15. 3% among patients with resumption of ovarian function.

The cumulative incidence of POF patients with resumption of ovarian function was 23% at 4 years, 28% at 10 years and 32% at 20 years after diagnosis in Kaplan–Meier analysis, 59% of the patients experienced this event in the first year of diagnosis.
 experienced an arrest of")
During the follow-up period of the 117 patients, 55 (47%) experienced an arrest of resumption of ovarian function. 1 year after resumption, 75% of the patients continued to have signs of ovarian function, 44% after 5 years and 26% after 10 years

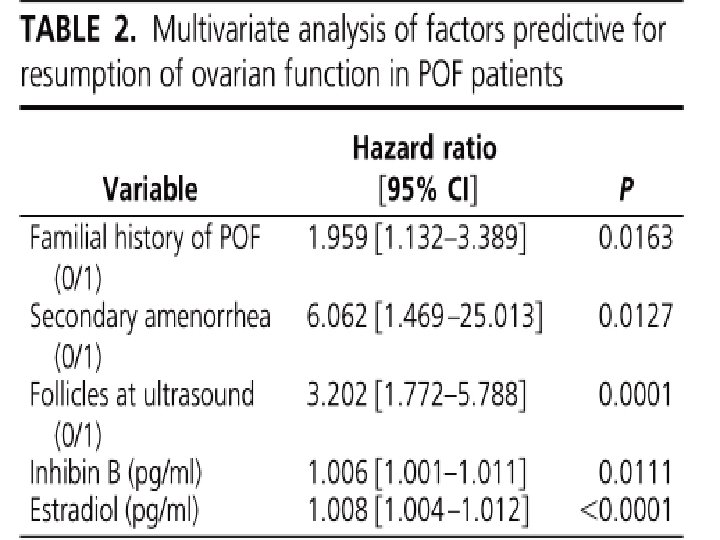
l Patients: A total of 358 consecutive POF patients were followed from 1997 to 2010 in an endocrinology center in Paris. l Main Outcomes Measures: The cumulative incidence of resumption of ovarian function was determined, and predictive factors were identified by univariate and multivariate analysis. J Clin Endocrinol Metab, December 2011, 96(12): 3864– 3872
 patients presented features indicating resumption of ovarian function, and in 77 cases")
86 (24%) patients presented features indicating resumption of ovarian function, and in 77 cases (88%) within 1 yr of diagnosis.

Take Home Message Diagnosis of POI should be based on a combination of oligomenorrhoea /amenorrhoea of more than 4 months’ duration associated with elevated gonadotropins (FSH >40 IU/l) on at least two occasions measured 4 -6 weeks apart in women under the age of 40. l AMH should not be routinely used to diagnose POI but may have a role when the diagnosis of POI is inconclusive. l

l Women with POI are at increased risk of cardiovascular disease, osteoporosis and cognitive impairment l Observational data have shown that women with POI have a lower risk of breast cancer compared with controls.

Systemic sex steroid hormone replacement is effective for the management of menopausal symptoms in women with POI and topical estrogen preparations are effective for the management of symptoms related to urogenital atrophy. l Sex steroid hormone replacement is likely to lower the long-term risk of CVD in women with POI, prevent osteoporosis and have a beneficial effect on cognitive function. l HRT does not appear to increase the risk of breast cancer in younger menopausal women under the age of 50. l

l HRT and the combined OCP would both be suitable options for hormone replacement, although HRT may be more beneficial in improving bone health and cardiovascular markers compared to the combined OCP.

THANK YOU FOR YOUR ATTENTION
- Slides: 84