A Mystery of Fracture By Dr Mitra Kazemi

A Mystery of Fracture By: Dr Mitra Kazemi Fellowship of endocrinology. Shahid Beheshti University of medical sciences

What is the mysterious cause of fracture in this patient?

Up To Date 2017

Up To Date 2017

Up To Date 2017

Is there any relationship between pregnancy and osteoporosis in this patient?

¨ Pregnancy and lactation associated osteoporosis is a rare condition in which women typically present with fractures, often vertebral, in the third trimester of pregnancy or in the early postpartum period. Obstet Gynecol Sci 2017; 60(1): 133 -137 https: //doi. org/10. 5468/ogs. 2017. 60. 1. 133 p. ISSN 2287 -8572 · e. ISSN 2287 -8580

¨ Some studies suggest that pregnancy is associated with bone losses of approximately 3% to 5% at the spine and hip. ¨ lactation has more consistent and profound effects on bone density. Bone loss of 3 to 10 percent at the spine and 2% to 4% at the hip are seen over 3 -6 months of lactation Obstet Gynecol Sci 2017; 60(1): 133 -137 https: //doi. org/10. 5468/ogs. 2017. 60. 1. 133 p. ISSN 2287 -8572 · e. ISSN 2287 -8580

¨ 1. calcium deficiency and hypoestrogenemia ¨ 2. endocrine changes during pregnancy ¨ 3. taking specific treatment, such as magnesium sulfate injection or prolonged bed-rest due to pregnancy induced hypertention or preterm labor Obstet Gynecol Sci 2017; 60(1): 133 -137 https: //doi. org/10. 5468/ogs. 2017. 60. 1. 133 p. ISSN 2287 -8572 · e. ISSN 2287 -8580

¨ 4. The relationship of obstetrical history and postpartum osteoporosis? ? ¨ 5. Genetic factors ¨ 6 Undoubtedly, lower BMD before pregnancy Obstet Gynecol Sci 2017; 60(1): 133 -137 https: //doi. org/10. 5468/ogs. 2017. 60. 1. 133 p. ISSN 2287 -8572 · e. ISSN 2287 -8580
, secreted by the lactating mammary gland, ¨ 8. Circulating calcitonin")
¨ 7. (PTHr. P), secreted by the lactating mammary gland, ¨ 8. Circulating calcitonin and the estrogen deficiency (the characteristic of lactation) Endocrinol Metab Clin N Am - (2016) -–http: //dx. doi. org/10. 1016/j. ecl. 2016. 09. 007

¨ Longitudinal studies in postpartum women show that recovery from lactationassociated bone loss may continue for 18 months or longer. ¨ Studies in both humans and animal models suggest that the pattern and extent of bone recovery may be site specific, with complete reversal at the spine but incomplete or slower recovery at other sites Endocrinol Metab Clin N Am - (2016) -–http: //dx. doi. org/10. 1016/j. ecl. 2016. 09. 007

¨ It usually presents in primigravid women, ¨ Rare recurrence of symptoms with subsequent pregnancies ¨ In women without a secondary cause, the usual course is complete resolution without recurrence Endocrinol Metab Clin N Am (2016) -–http: //dx. doi. org/10. 1016/j. ecl. 2016. 0 9. 007

But what about The Juenile Osteoporosis?

¨ Idiopathic juvenile osteoporosis is a rare disease affecting children between 8 and 14 years of age. ¨ The pathogenesis of the disease has not been completely established ¨ Once all of the known causes of decreased bone mass are excluded, there remains one form of osteoporosis over IJO

It was first recognized by Dent in 1965 Due to the rare prevalence of Idiopathic Juvenile Osteoporosis, only approximately 100 cases have been reported in the literature, and its descriptions have been limited to case reports

¨ No heritable genetic mutations have been identified in patients with IJO ¨ Absence of family members with a history of pediatric or adolescent osteoporosis suggests IJO. ¨ It is self restrictive and shows marked, spontaneous improvement during adolescence.

…and finally what about the Idiopathic Osteoporosis? ?

¨ The term idiopathic osteoporosis applies only to the premenopausal women with a history of low trauma fractures who has no known secondary cause after extensive evaluation , and not to those with low BMD and no Hx of Fx Curr Osteoporos Rep (2013) 11: 276– 285

¨ It has been reported predominantly in Caucasians, ¨ family history of osteoporosis is common. ¨ A heterogeneous disorder, Curr Osteoporos Rep (2013) 11: 276– 285 DOI 10. 1007/s 11914 -013 -0161 -4
 levels, ¨ Those with high")
¨ Those with low bone turnover had higher (IGF-1) levels, ¨ Those with high bone turnover manifested a biochemical pattern suggestive of primary/idiopathic hypercalciuria Curr Osteoporos Rep (2013) 11: 276– 285 DOI 10. 1007/s 11914 -013 -0161 -4

So the diagnosis maybe the Idiopathic Osteoporosis

Management ¨ For all patients, it is appropriate to recommend a set of general measures that benefit bone health. Such measures include getting adequate amounts of weight-bearing exercise, protein, calories, calcium, and vitamin D, as well as lifestyle modifications Curr Osteoporos Rep (2013) 11: 276– 285 DOI 10. 1007/s 11914 -013 -0161 -4

¨ In premenopausal women with isolated low BMD and no history of fractures, in whom no secondary cause can be identified, pharmacological therapy is rarely necessary. BMD should be remeasured after 1 or 2 years to identify women with declining BMD Curr Osteoporos Rep (2013) 11: 276– 285 DOI 10. 1007/s 11914 -013 -0161 -4

Bisphonates ¨ Bisphonates carry a Category C rating for safety in pregnancy, because they accumulate in the skeleton, cross the placenta and have been reported to cause toxic effects in pregnant rats. ¨ Effective contraception should be encouraged during bisphonate use, there is also the potential for adverse effects after stopping bisphonates, since ¨ they remain in the skeleton for years. Curr Osteoporos Rep (2013) 11: 276– 285 DOI 10. 1007/s 11914 -013 -0161 -4

So what about Teriparatide? ?

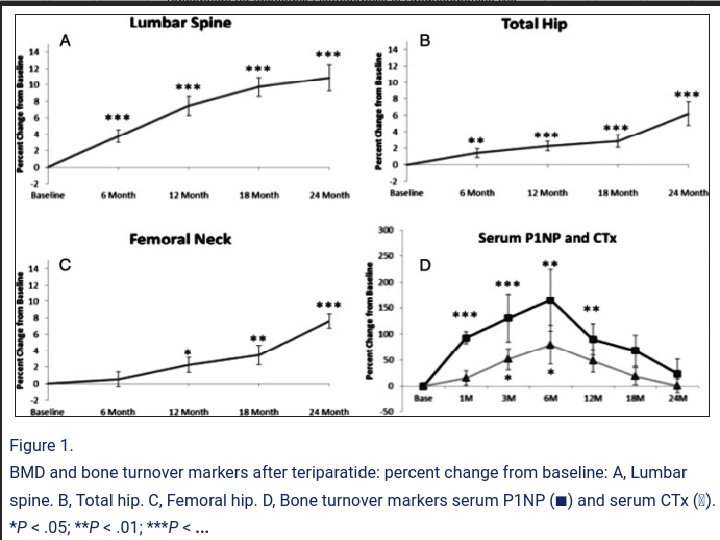
Methods: This was an open-label pilot study. Participants were 21 premenopausal women with unexplained fragility fractures or low BMD. Teriparatide was administered at 20 μg daily for 18 to 24 months J Clin Endocrinol Metab. 2013 May; 98(5): 1971– 1981. Published online 2013 Mar 29. doi: 10. 1210/jc. 2013 -1172

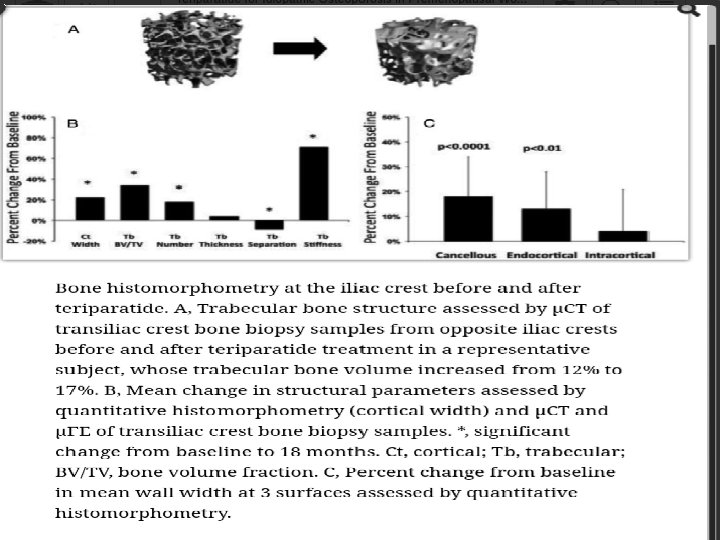
¨ The primary endpoint was within-subject percent change in lumbar spine BMD. Secondary endpoints included: percent change in hip BMD, transiliac biopsy parameters, serum (P 1 NP), and Ctelopeptide. J Clin Endocrinol Metab. 2013 May; 98(5): 1971– 1981. Published online 2013 Mar 29. doi: 10. 1210/jc. 2013 -1172

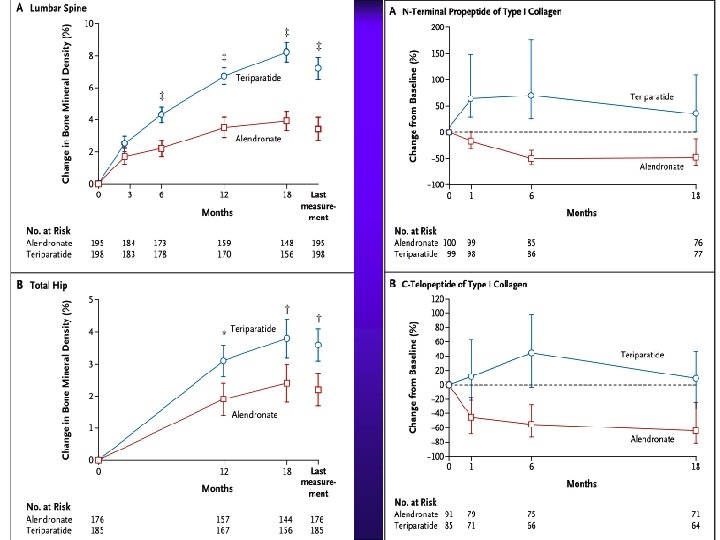
Methods: ¨ In an 18 -month randomized, double-blind, controlled trial, we compared: ¨ teriparatide with alendronate in 428 women and men with osteoporosis (ages, 22 to 89 years) who had received glucocorticoids for at least 3 months (prednisone equivalent, 5 mg daily or more). N Engl J Med 2007; 357: 2028 -39. Copyright © 2007 Massachusetts Medical Society.

¨ A total of 214 patients received 20 μg of teriparatide once daily, and 214 received 10 mg of alendronate once daily. ¨ The primary outcome was the change in BMD at the lumbar spine. ¨ Secondary outcomes included changes in BMD at the total hip and in markers of bone turnover, the time to changes in BMD, the incidence of fractures, and safety, N Engl J Med 2007; 357: 2028 -39. Copyright © 2007 Massachusetts Medical Society.

So it seems that Teriparatide maybe better than Bisphonates in this patient!

But what about the risk of the future fractures in this patient?
 who were 10 or")
Cross sectional study of 1284 women (mean age 73 years) who were 10 or more years postmenopausal, detailed information on their fracture, medical, menstural, alcohol and smoking histories was obtained using a standardized questionarie

¨ Artic; e FX 2

Methods: We obtained information about any lifetime fractures of the hip, arm, spine, wrist, leg, ankle, foot and finger from 9086 ambulatory white women ages 65 years and older participating in the Study of Osteoporotic Fractures. Osteoporos Int (2002) 13: 337– 341 2002 International Osteoporosis Foundation and National Osteoporosis Foundation

¨ We also measured BMD and recorded history of falls, maternal fracture history, drug use, diet, functional status, and other characteristics commonly associated with osteoporotic fractures. Osteoporos Int (2002) 13: 337– 341 2002 International Osteoporosis Foundation and National Osteoporosis Foundation

¨ Women with a premenopausal fracture were about 35% more likely to have a fracture during the SOF study period than women without a premenopausal fracture (47. 7 Fx /1000 person-years vs 35. 1 Fx/1000 person-years, p=0. 001).

But what about the role of BMD in this patient?

Since there are few longitudinal prospective studies relating BMD by DXA to fracture risk in premenopausal women and because fracture rates are much lower in premenopausal than postmenopausal women, Screening BMD by DXA is not recommended in premenopausal women. Endocrinol Metab Clin N Am (2016) -–http: //dx. doi. org/10. 1016/j. ecl. 2016. 0 9. 007

BMD measurement is recommended: ¨ In young women with a history of low trauma fracture and ¨ In those with known causes of bone loss Endocrinol Metab Clin N Am (2016) -–http: //dx. doi. org/10. 1016/j. ecl. 2016. 0 9. 007
 recommends use of BMD Z scores rather than T scores at")
¨ The (ISCD) recommends use of BMD Z scores rather than T scores at the lumbar spine, hip, and forearm in premenoopausal women ¨ Z score less than or equal to 2. 0 : “below the expected range for age” ¨ and a Z score greater than 2. 0 : “within the expected range for age. ” Endocrinol Metab Clin N Am - (2016) -–http: //dx. doi. org/10. 1016/j. ecl. 2016. 09. 007

Thank You For Your Attention
- Slides: 55