Diagnosis of Deception How Semicircular Canal Dehiscence Masquerades










. The dura")


- Slides: 14
Diagnosis of Deception: How Semicircular Canal Dehiscence Masquerades as a Psychiatric Disorder Bree Smouse, MD and Kevin Ozment, MD ACP Resident Members National Jewish Health – St. Joseph Hospital May 14 th 2019 ACP Colorado Chapter Residents/Fellow Meeting
Case Presentation CHIEF COMPLAINT: 34 year old F hearing “odd noises”, insomnia, anxiety HPI • Presented to behavioral health at age 20, diagnosed with GAD and rx SSRIs • Progression of symptoms – Grinding noises when turning head side to side or when moving other joints such as elbows – “Squishing sound” when blinking eyes – Heart beat sounds amplified in her head
Case Presentation • Diagnosed with bipolar affective disorder due to depression and insomnia • Progression of symptoms in 2018 – Ordinary noises such as a knock on the door caused vertigo – Earplugs needed just to go outside • Sent for audiology eval and vestibular-evoked myogenic potential testing showed vestibular activation by loud sounds
Case Presentation PMHx: Multiple sclerosis, Crohn’s disease, depression, bipolar II PSHx: None Family Hx: Unknown, patient was adopted Medications: Hydroxyzine, mesalamine, fluoxetine, trazodone Social Hx: • Former smoker, quit 2013 • No alcohol use • Daily marijuana
Case Presentation Vitals: Afebrile, HR 79, BP 104/61, RR 18, O 2 100% on RA Physical Exam HEENT – normal external auditory canals/ears, normal appearing TM’s b/l Neuro – decreased air conduction and increased bone conduction with Rinne Labs Unremarkable
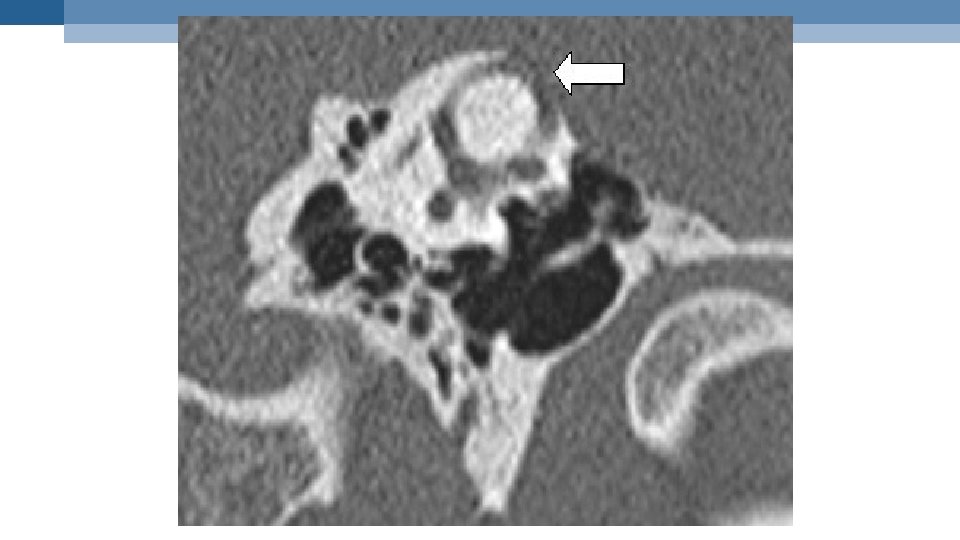
Disease Course • Sub-millimetric temporal bone CT supported diagnosis of bilateral superior canal dehiscence syndrome • Scheduled for right sub-temporal craniotomy with neurosurgery to repair the defect in the right semicircular canal • Procedure performed 12/14/18 • Brief routine stay in ICU for post-operative management followed by discharge home
Post-op follow up Neurosurgery note 1/22/19 “She is doing well post-operatively with near complete resolution of her preoperative symptoms. Her right-sided symptoms have essentially resolved, but she still have some mild autophony on the left and can heartbeat. She is starting to wonder if she needs to treat the left side as well. Overall she is doing very well and very happy with the results. ”
Superior Canal Dehiscence Syndrome
Symptoms • Chronic disequilibrium • Autophony – “Hearing” eye movements, breathing, chewing, creaking joints, digestive noises or pulse Pulsatile oscillopsia Pulsatile tinnitus Tullio phenomenon Hypersensitivity to bone-conducted sounds • Conductive hearing loss for low frequency sounds • Fatigue/Migraine/headache/Aural fullness • • Triggers • Loud noises • Pressure applied to outside ear (even laying on a pillow) • Increase in ICP (eg: sneezing, bearing down, nose-blowing. )
Causes • Likely a developmental abnormality of the tegmen – Up to 1 -2% of the population have the abnormality – Primarily congenital phenomenon, possibly acquired – Incidence unknown • The section of temporal bone develops to only 60% of normal thickness and then is eroded away by: – Head trauma – Pressure-altering events (eg: diving) – Age
Surgical Correction The dehiscence is clearly visualized using a micro-endoscope (black arrow). The dura is carefully elevated from the underlying semicircular canal in preparation for resurfacing (yellow arrow). The cartilage graft is placed into the mini-craniotomy site and used as a cap over the superior semicircular canal dehiscence (black arrow).
Take aways from this case Misunderstood in health care: – Often misdiagnosed for years (told they have ear wax, fluid in the ear, orthostatic hypotension, etc. ) – In some instance patient’s are told that they just have anxiety or in this case, are diagnosed with depression, anxiety or other mental illness – Can be socially isolating – Easily treatable (94% surgical success rate)
Thank you! Questions? • Cloutier J. -F. , Belair M. , Saliba I. Superior semicircular canal dehiscence: positive predictive value of high-resolution CT scanning. Eur. Arch. Otorhinolaryngol. 2008; 265(12): 1455 -1460 • Ohman, Jenny et al. Patients’ experiences of living with superior canal dehiscence syndrome. International Journal of Audiology. Seept 2018; 825 -830. • Ward, Bryan and Carey, John. Superior Canal Dehiscence Syndrome: Lessons from the first 20 years” Frontiers of Neurology. Apr 2017; 8: 177. Bree. smouse@sclhealth. org Kevin. ozment@sclhealth. org