1 FASCIAL DEHISCENCE FASCIAL DEHISCENCE Fascial disruption is

















 with permanent or")



")








- Slides: 33
1
FASCIAL DEHISCENCE
FASCIAL DEHISCENCE Fascial disruption is due to abdominal wall tension overcoming tissue or suture strength, or knot security. It can occur early or late in the postoperative period, and involve a portion of the incision (ie, partial dehiscence) or the entire incision (ie, complete fascial dehiscence).
FASCIAL DEHISCENCE • With early fascial dehiscence, the skin closure may be intact depending upon the method of closure (ie, staples, sutures); the patient, nevertheless, is at risk for evisceration. Early postoperative fascial dehiscence is a surgical emergency. • The late complication of fascial disruption is incisional hernia.
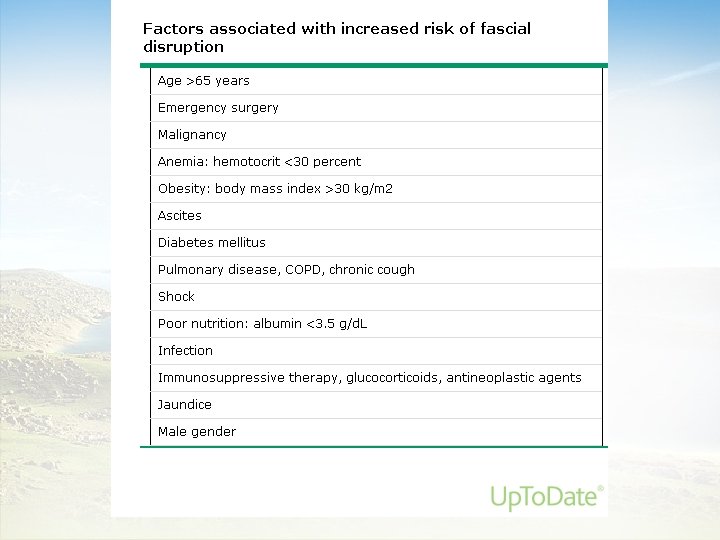
Risk Factors
Risk Factors • Technical factors — Fascial dehiscence may also be related to technique. • Incisional factors — Tension on an incision is proportional to its length. Herniation is more common when the incision length exceeds 18 cm. It was thought that longitudinal incisions were at greater risk of dehiscence than transverse incisions but. .
Risk Factors • Suture — The main causes of wound separation are failure of suture to remain anchored in the fascia, suture breakage, knot failure, and excessive stitch interval which allows protrusion of viscera.
Risk Factors • In up to 95 percent of abdominal wound dehiscences, the sutures and knots are intact, but the suture has pulled through the fascia. This is usually the result of fascial necrosis from sutures being placed too close to the edge or under too much tension.
Risk Factors • Sutures should be about 1 cm from the wound edge and about 1 cm from the adjacent suture to ensure that the tissue is strong enough to hold the suture. • For continuous closure, the total length of the suture should be approximately four times the length of the incision.
Clinical manifestations and diagnosis
Clinical manifestations and diagnosis • Signs and symptoms of a complete dehiscence include profuse serosanguinous drainage, often preceded by a popping sensation and an incisional bulge exacerbated by Valsalva maneuvers. • Most dehiscences occur 4 to 14 days after surgery, with a mean of 8 days.
Treatment
Treatment • When fascial disruption is suspected, wound exploration should be performed in the operating room. Complete fascial dehiscence is associated with a mortality rate of 10 percent, and is a surgical emergency.
Treatment • At the bedside, a moist dressing is placed over the wound a binder can be placed around the patient's abdomen to prevent overt evisceration on the way to the operating room. A binder should not be used in cases of complete dehiscence and evisceration due to the potential for bowel injury.
Treatment • Once the wound is opened, the edges are thoroughly debrided. • A mass closure with continuous, slowly absorbable suture should be performed. Depending upon the circumstance, the skin may or may not be left open.
Prevention
Prevention ●Use of a simple running technique ●Use of #1 or #2 delayed absorbable suture ●Use of mass closure to incorporate all layers of the abdominal wall (except skin) ●Taking wide tissue bites (about 1 cm) ●Use of a short stitch interval (about 1 cm) ●Use of a suture length to wound length ratio of 4 to 1 ●Use of non-strangulating tension on the suture
Prevention • Continuous mass closure or interrupted Smead-Jones closure (vertical mattress) with permanent or delayed absorbable suture are both safe and effective. • Most midline closures should be performed with continuous mass closure supported by several recent metaanalyses.
SSIs
SSIs • Surgical wound infections are a common cause of nosocomial infection. The United States Centers for Disease Control and Prevention (CDC) has developed criteria that define surgical site infection (SSI) as infection related to an operative procedure that occurs at or near the surgical incision within 30 days of the procedure, or within 90 days if prosthetic material is implanted at surgery.
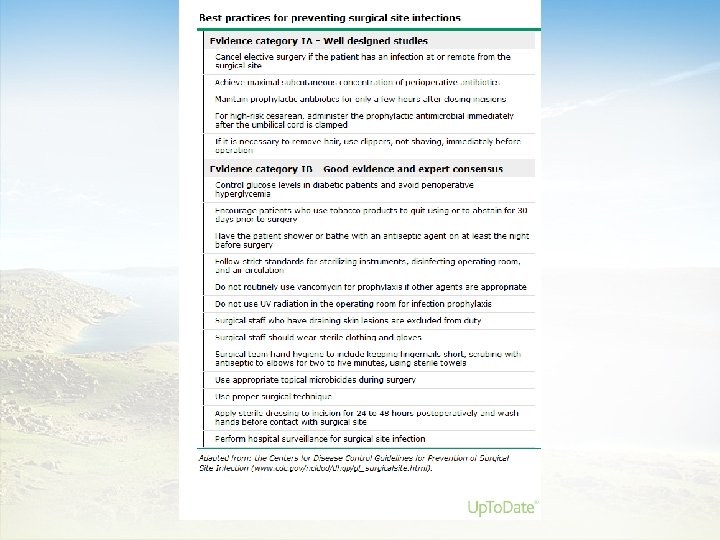
SSIs Risk Factors
SSIs Risk Factors that may impact the rate of SSIs (apart from antimicrobial prophylaxis) include : ●Attention to basic infection control strategies ●Surgical technique ●Prolonged duration of surgery ●Hospital and operating room environments ●Instrument sterilization ●Preoperative preparation (surgical scrub, skin antisepsis) ●Perioperative management (thermoregulation, glycemic control) ●Underlying medical condition of the patient
SSIs Risk Factors Several factors related to the surgical environment and operative practices have been identified as risk factors for SSI. These include: ●Preoperative hair removal (particularly shaving) ●Inordinate personnel traffic during an operation ●Excessive use of electrosurgical cautery units ●Presence of a prosthesis or other foreign body ●Degree of tissue trauma ●Need for blood transfusion
SSIs Risk Factors Several other patient characteristics have been identified as risk factors for SSI, including : ●Age ●Diabetes ●Obesity ●Cigarette smoking ●Immunosuppression ●Malnutrition ●Preoperative colonization with potentially pathogenic microorganisms ●Presence of infection at a nonsurgical site ●Recent surgery ●Duration of preoperative hospitalization ●Severity of underlying illness(es)
Prophylaxis
Prophylaxis • Antibiotic prophylaxis should be administered in doses sufficient to achieve adequate serum and tissue drug levels for the interval during which the surgical site is open. For most adults, it is acceptable to dose antimicrobials based on standardized doses for safety, efficacy, and convenience. However, the serum and tissue concentrations of some drugs administered to obese patients may differ from those in nonobese patients for a number of reasons, including pharmacokinetic variability related to the lipophilicity of the administered drug.
Prophylaxis • Timing — Antimicrobial therapy should be completely infused 60 minutes prior to surgical incision, if possible, to optimize adequate drug tissue levels at the time of initial incision.
Prophylaxis • Administration of vancomycin or a fluoroquinolone should begin 120 minutes before surgical incision because of the prolonged infusion times required for these drugs. Some studies suggest lower infection risk with initiation of antimicrobial administration within 30 minutes before surgical incision, although thus far data are insufficient to support this approach as a routine practice. • If the 60 -minute window for prophylaxis has passed, antimicrobial administration 30 to 60 minutes prior to incision appears to be more effective than administration immediately before surgical incision.
Prophylaxis • Repeat dosing — To ensure adequate antimicrobial serum and tissue concentrations, repeat intraoperative dosing is warranted for procedures that exceed two half-lives of the drug and for procedures in which there is excessive blood loss (>1500 m. L).
Prophylaxis • Duration — In general, repeat antimicrobial dosing following wound closure is not necessary and may increase the risk for development of antimicrobial resistance. • For cases in which prophylaxis beyond the period of surgery is warranted, in general, the duration should be less than 24 hours.