UPDATES AND RECENT CONTROVERSY IN TREATMENT OF LOWER





 • PT – flexion based or")

 • Radiofrequency current used to create heat. • 85 degrees")




 • Utility of a corticosteroid injection")













 3 months after")







 EVIDENCE SUPPORTING LUMBAR RFA • Evidence is variable due to two important considerations:")



- Slides: 39
UPDATES AND RECENT CONTROVERSY IN TREATMENT OF LOWER BACK PAIN Benjamin Bonte, MD Interventional Pain Fellow Hudson Spine & Pain Medicine 8/30/2017
JOINT DISORDERS AND DISC PAIN • Lumbar Facet arthropathy • SIJ pain • Discogenic pain • Controversial Dutch Neurotomy Study (Juch et al)
JOINT DISORDERS AND DISC PAIN • Lumbar Facet arthropathy • SIJ pain • Discogenic pain • Controversial Dutch Neurotomy Study
LUMBAR FACET ARTHROPATHY • Facet joints are synovial joints that sustain progressively increasing loads down the spine, reaching 12 -25% body weight in the lumbar region. • As disc height decreases (age, trauma), progressive load is placed on facet joint • Lumbar facet hypertrophy can lead to central canal and lateral recess/foraminal stenosis • i. e. radiculopathy can coexist with this pathology
FACET ARTHROPATHY • Pain worse with oblique movements and extension • Referred pain pattern can be seen • Pure facet pain should not have neurologic abnormalities • Imaging – XR, CT, MRI
TREATMENT • Rest, pain control (NSAIDs, muscle relaxants) • PT – flexion based or neutral postures, proper body mechanics • Injections, RFA
TREATMENT Z-JOINT INJECTION • Mostly for therapeutic purposes • As anesthetic can easily spread to nerve root, may not allow to distinguish between facet<>radicular pain MEDIAL BRANCH BLOCK • Performed for diagnostic reasons to confirm pain generator. • Precursor for RFA • No reported complications
LUMBAR RADIOFREQUENCY ABLATION (RFA) • Radiofrequency current used to create heat. • 85 degrees C, 90 seconds • Lesion is produced along the length of the noninsulated tip, so needle placement parallel to nerve is ideal • Painful, thus conscious sedation is typical • Stimulation used to rule out placement near the nerve root/DRG • Complications are rare • Local pain or neuritic pain lasting >2 weeks is 0. 5%
EVIDENCE SUPPORTING LUMBAR RFA • Evidence is variable due to two important considerations: 1. Patient Selection • Studies that set the bar low for RFA have less success. • Single blocks, or low % relief from block • Van. Kleef - Patients fare worse, 50% pain relief in 46% of RFA group vs 12% controls • Some studies show no benefit • When strict inclusion criteria are used, results are better. • Dreyfuss et al – 60% of patients had +90% pain relief. 87% of patients had +60% relief. • Nath et al – 40 patients (20/20) inclusion = 3 diagnostic blocks. RFA –statistically significant improvement in pain, QOL 2. Technique • Larger probes with longer active tips are more likely to denervate the medial branch. • Dreyfuss – 16 g, 5 -mm tip (2 contiguous lesions with goal of 10 mm lesion) • Nath - 22 g, 5 -mm tip (2 contiguous lesions with goal of 10 mm lesion), made at 3 different locations for each medial branch
JOINT DISORDERS AND DISC PAIN • Lumbar Facet arthropathy • SIJ pain • Discogenic pain • Controversial Dutch Neurotomy Study
JOINT DISORDERS AND DISC PAIN • Lumbar Facet arthropathy • SIJ pain • Discogenic pain • Controversial Dutch Neurotomy Study
SI JOINT PAIN • Synovial joint anteriorly and syndesmosis posteriorly. • L 5 dorsal ramus and lateral S 1 -S 3 dorsal rami • Typically 6 provocation tests are used in academic literature (distraction, compression, thigh thrust, gaenslen’s, FABER, Sacral thrust) • If none are positive, SIJ can be ruled out. • If 3+ are positive, then PPV of SIJ pain is 77% • Still, the only accepted method of diagnosing this pain is with a diagnostic injection.
TREATMENT • Trial of noninterventional care (PT, medications) • Utility of a corticosteroid injection is debatable except in cases of sacroiliitis. Generally a diagnostic procedure.
EVIDENCE • Multiple RCTs show benefit from intraarticular steroids in sacroiliitis. No conclusive evidence for other reasons of SIJ pain. • Optimal RFA results occur when there is very stringent selection criteria. • Cohen + Abdi • 18 subjects with 80% relief with SIJ block. • 9 had 50% relief from L 4 MBB, L 5 DR, and S 1 -S 3 LBB. All underwent RFA • 8 of 9 had >50% relief for duration of 9 months. • Technical success maximized with parallel needle placement, larger gauge needle, and multiple lesion technique.
JOINT DISORDERS AND DISC PAIN • Lumbar Facet arthropathy • SIJ pain • Discogenic pain • Controversial Dutch Neurotomy Study
DISCOGENIC PAIN • irritation of the annulus and PLL, with innervation from sinuvertebral nerve and/or somatic afferent nerves • Worse with lumbar flexion as this increases intradiscal pressure
DIAGNOSIS AND EVIDENCE FOR TREATMENT • Provocation discography with balloon tipped intradiscal catheters, followed by anesthetic injection to the disc with 50%+ reduction in pain has better response to interbody fusion surgery than use of standard contrast studies. • Intradiskal electrothermal therapy (IDET), radiofrequency therapy are procedures that require further study, with some studies showing benefit/decreased cost as compared to surgery.
JOINT DISORDERS AND DISC PAIN • Lumbar Facet arthropathy • SIJ pain • Discogenic pain • Controversial Dutch Neurotomy Study
CONTROVERSIAL DUTCH NEUROTOMY STUDY
OBJECTIVE • To evaluate the effectiveness of RF denervation added to a standardized exercise program for patients with chronic low back pain
IMPORTANCE OF THE STUDY • Low back pain is the #1 leading cause of disability with tremendous effects on quality of life and healthcare spending • Estimated costs in the US have been estimated at $87 b over 17 years (1996 -2013) • Mechanical low back pain (facet joints, SI joints, intervertebral discs) is frequently treated with RF; low to moderate quality evidence has been demonstrated in the past to show effectiveness
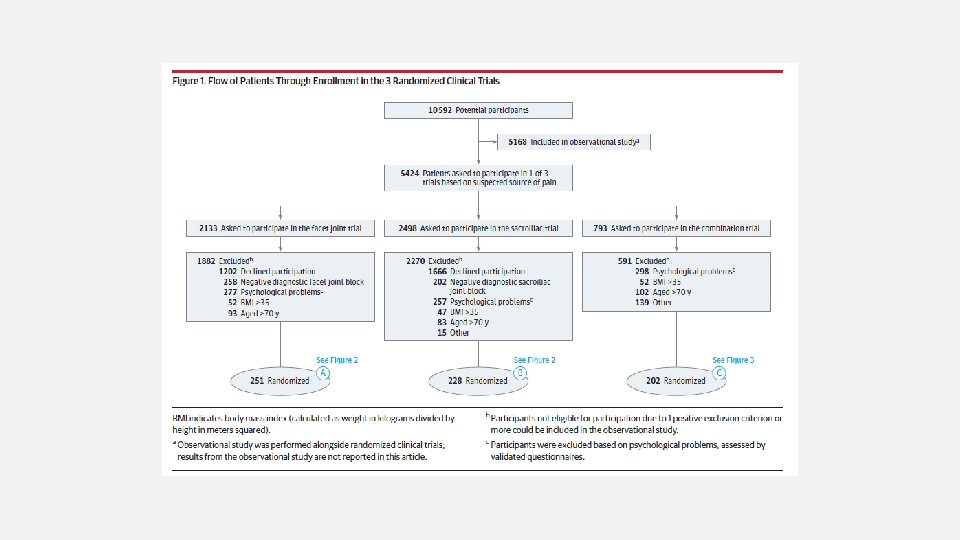
STUDY DESIGN • 3 randomized clinical trials with 681 participants • Chronic low back pain originating from • Facet joints • SI joints • Combination – combination of facet, SI, or intervertebral disc • (Intervertebral disc alone - terminated due to lack of eligible participants)
INCLUSION CRITERIA • Pain related to facet, SI, or intervertebral disc • Source – determined by clinical examination • Facet – clinical examination + facet block; included in randomization if this was positive. • SI – positive in at least 3 of 6 provocation tests qualified for a block, then included if this was positive. • Compression test, distraction test, FABER, Gaenslen, thigh thrust, Gillett • Mixed – (facet, SI, or intervertebral disc) – 1 block; included if positive, 2 nd block if first negative, 3 rd block if 2 nd negative. • Positive = 50% pain reduction within 30 -90 minutes after the block, after injecting the areas with 2% lidocaine (0. 5 ml). For disc, pressure controlled discography and 1 negative control level. • Age 18 -70 • No improvement in symptoms after conservative treatment
EXCLUSION CRITERIA • Pregnancy • Severe psychological problems • Involvement in work-related conflicts/claims • BMI >35 • Age >70 • On anticoagulant therapy or with coagulopathy
OTHER INTERVENTIONS • All received a physical therapy program • Randomized participants received radiofrequency denervation with 22 g needle (full technical details not included in main article – next slide) • Cointerventions were not allowed • Surgery, manual therapy, chiropractic therapy, new medications. • OTC meds allowed • Radiofrequency denervation was allowed after 3 months. • Psychological care was not considered a co-intervention
RFA TECHNIQUE
OUTCOME MEASUREMENTS • Primary outcome • Pain from 0 -10 (NRS) 3 months after the intervention • Clinically important difference was 2 points or more. • Secondary outcomes • Perceived recovery, patient satisfaction, functional status, QOL • Data collection at 3, 6, 9, 12 month follow-up intervals, through web-based questionnaires.
RESULTS – FACET JOINT TRIAL • 251 patients ultimately included in facet joint trial • 123 in the intervention group, 126 in the control group • Similar group composition however first episode of LBP was 12 years prior compared to 8 years prior in control group. • No significant differences between groups were found when success was defined as more than 30% or 2 point reduction in pain at 3 months. • Mean age 52. 2 years. • 61. 8% female • Mean baseline pain intensity of 7. 1
RESULTS – SIJ TRIAL • 228 patients included in the SIJ trial • 116 in the intervention group / 112 in the control group • First episode of LBP was 97 months compared with 65 months on control group • No significant differences in outcome found when success was defined as more than 30% or 2 points reduction or more in pain at 3 months.
RESULTS – COMBINATION TRIAL • 202 patients in the combination trial • 103 in the intervention group / 99 in the control group • Statistically significant difference in outcome found when success was defined as more than 30% or 2 points reduction or more in pain at 3 months.
DISCUSSION • Radiofrequency denervation is not recommended and patients with chronic LBP with no improvement in symptoms after conservative treatment have no clear alternative therapies. • Strengths • Sample size, good randomization, outcome measures, followup duration of 12 m • Some Key Limitations • Different SIJ RFA techniques were used (cooled RF, palisade, simplicity III) • Not blinded • Threshold value for a “positive block” • Exclusion of patients with psychological problems may affect how generalizable results are
POINTS OF CONTROVERSY
INHERENT BIAS • this unblinded study was funded in part by grant money received from Dutch health insurance companies
INADEQUATE DIAGNOSTIC ASSESSMENT • many patients treated with RFN likely did not have facet joint or sacroiliac joint pain, and would not have been expected to experience pain relief or functional improvement. • Inclusion criteria (from prior slide) • Source – determined by clinical examination • Facet – clinical examination + facet block; included in randomization if this was positive. • SI – positive in at least 3 of 6 provocation tests qualified for a block, then included if this was positive. • Compression test, distraction test, FABER, Gaenslen, thigh thrust, Gillett • Mixed – (facet, SI, or intervertebral disc) – 1 block; included if positive, 2 nd block if first negative, 3 rd block if 2 nd negative. • Positive = 50% pain reduction within 30 -90 minutes after the block, after injecting the areas with 2% lidocaine (0. 5 ml). For disc, pressure controlled discography and 1 negative control level.
(AGAIN) EVIDENCE SUPPORTING LUMBAR RFA • Evidence is variable due to two important considerations: 1. Patient Selection • Studies that set the bar low for RFA have less success. • Single blocks, or low % relief from block • Van. Kleef - Patients fare worse, 50% pain relief in 46% of RFA group vs 12% controls • Some studies show no benefit • When strict inclusion criteria are used, results are better. • Dreyfuss et al – 60% of patients had +90% pain relief. 87% of patients had +60% relief. • Nath et al – 40 patients (20/20) inclusion = 3 diagnostic blocks. RFA –statistically significant improvement in pain, QOL 2. Technique • Larger probes with longer active tips are more likely to denervate the medial branch. • Dreyfuss – 16 g, 5 -mm tip (2 contiguous lesions with goal of 10 mm lesion) • Nath - 22 g, 5 -mm tip (2 contiguous lesions with goal of 10 mm lesion), made at 3 different locations for each medial branch
INEFFECTIVE TECHNIQUE SELECTION • Small lesions with 22 g needle most likely missed many targeted nerves and would not be expected to relieve pain from the lumbar facet joints.
THANK YOU!
PROCEDURE FOR INTRADISCAL RFA