UCSD SKIN ASSESSMENT DOCUMENTATION Cheryl Garnica RN CWOCN


 Medicare payment changes: Stage III")



































 Measureable outcomes/Realistic Interventions: specific for patient vs.")






- Slides: 50
UCSD SKIN ASSESSMENT & DOCUMENTATION Cheryl Garnica RN, CWOCN Spring 2011
SKIN TRENDS AND REGULATION CHANGES 2007: Changes by CMS for payment of HAPUs NUAP new definitions for pressure ulcers Addition of Pressure Ulcer Stages: Unstageable and Deep Tissue Injury 2009: Clarification of MMPs (mucous membrane pressure ulcers: do not fit in staging guidelines Best practice/evidence based guidelines published by NPUAP and EPUAP
REGULATION & REPORTING CHANGES POA defined (Present on Admit) Medicare payment changes: Stage III , Stage IV, Deep Tissue injuries and unstageable HAPUs: Possibly no $$monetary compensation CDPH: MUST be notified within 5 days of finding HAPPU Stage III, IV, Unstageable and DTI present on admit that converts to unstageable eschar
Who Stages Pressure Ulcers? ? ANA position Statement 2010: Nurses!! BUT: you must be able to differentiate between pressure ulcers and other types of wounds Physicians
RESOURCES FOR SKIN CARE AT UCSD Skin Team Champion CNS/Clinical Nurse Educator WOCN MD Wound Manual Skin Standards on Web Ref Cal Noc Tutorial: User ID: tuto 620 Password: tuto 634 www. nursingquality. org PU learning modules
Skin Facts Largest organ Often reflects patient’s general condition First line of defense against moisture, pathogens Thermoregulation Sensory Metabolism (Vit. D) Communication
Changes with aging Less fat, collagen: decreased elasticity Decreased sensation Decreased thermoregulation Decreased ability to fend off pathogens
Factors that alter skin integrity Nutrition Age Disease State Hydration Medications Sensory Impairment Mental Impairment Immobility Incontinence Circulation
SKIN: NURSES RESPONSIBILITY Promote and maintain skin integrity Assess and Identify risk factors: for skin impairment Implement Interventions: to prevent skin breakdown Document: findings & interventions Communicate: to physicians and staff Educate: family re: Breakdown prevention and treatment
Skin Assessment: Frequency On admit, within first hour Every shift Transfer to unit Change in condition or level of care Post procedure Reassessment: every position change
Methods of Skin Inspection Visual and Touch Head to toe inspection Particular attention to boney prominences: occiput, spine, shoulder blades, elbows, sacrum, coccyx, heels, trochanters, Maleolus, ischeum In skin folds (especially with Bariatric patients) Check under medical devices
Pressure points to check
What to assess? ? Color: blanchable, pale, redness; dark skin may require flashlight for assessing at risk pressure areas Intact or not? Turgor (resilience, hydration) Temperature: warm, cold Moisture: incontinent, sweating, dry, flakey Texture: hard, soft, boggy, mushy, induration, blistering Existing skin issues: wounds, rashes, bruises, skin tears, ecchymosis
BRADEN SCALE Identifies Risk Factors Contributing to Skin Breakdown Sensory Moisture Activity Mobility Nutrition Friction and Shear 18 or less: MUST HAVE CARE PLAN
BRADEN SCALE: Completed every shift and on change in condition or level of care Low scores on Braden subscale: should drive your care plan and interventions for skin care
FINDINGS ON ASSESSMENT Skin alterations, open wounds: Identify source (pressure, skin tear, shear, abrasion, surgical wound, venous or arterial ulcers, trauma, etc. Get a history from the patient Describe what you see
Is it a pressure ulcer? Definition: Damage caused to skin and underlying soft tissue by unrelieved pressure when the tissue is compressed between a bony prominence and external surface over a prolonged period of time 3 main contributing factors in formation: Pressure, Shear and Friction Most pressure ulcers are over a bony prominence, however, they may be present over soft tissues. Keypoint: assess over bony areas AND under medical devices (SCDs, oxygen prongs and tubings, foleys, drains, objects left in bed, etc. )
STAGE I Intact skin with non-blancheable redness of a localized area usually over a boney prominence. Darkly pigmented skin may not have visible blanching; its color may differentiate from the surrounding area. Keypoint: dark skin individuals: inspect skin for warmth, coolness, induration (firm, hard) or boggy areas. May be painful.
Stage I
Stage II Partial thickness loss of dermis which may present as a shallow crater, NO SLOUGH (yellow dead tissue). May also present as a serum filled blister (intact or ruptured). Keypoint: dermal depth, all pink, shallow; do not use Stage II to define skin tears
Stage II
Shear effect with pressure
Stage III Full thickness tissue loss. Subcutaneous fat may be visible. Bone, tendon or muscle NOT exposed. Slough may be present, but does NOT obscure the depth of tissue loss. May include undermining and tunneling. Keypoint: amount of subcutaneous tissue varies per anatomical area and per individual. Thin folks: little subcutaneous tissue whereas morbidly obese may have excess
Stage III
Stage IV Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present on some parts of the wound bed. Often include undermining and tunneling. Keypoint: Depth of tissue loss varies per anatomical location. Bridge of nose, ear, occiput and malleolus have little or no subcutaneous tissue; these Stage IV ulcers CAN BE SHALLOW
Stage IV
Unstageable Full thickness tissue loss in which the base of ulcer is covered by slough (yellow, tan, gray, green, brown) and/or eschar (tan, brown or black) in the wound bed. Keypoint: until enough slough/eschar is removed to expose the base of the wound, you can not accurately stage it; therefore, it is unstageable
Unstageable
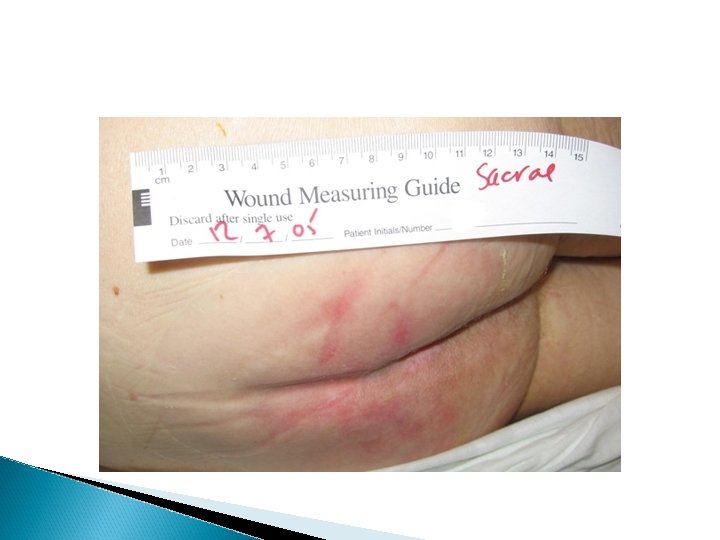
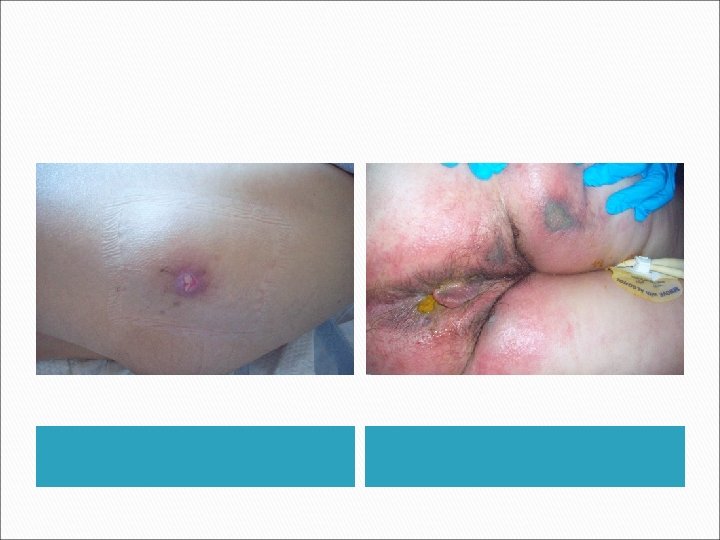
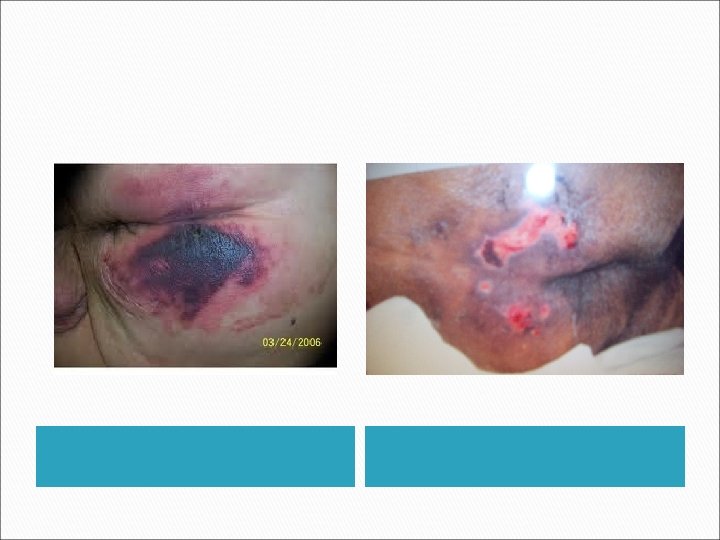
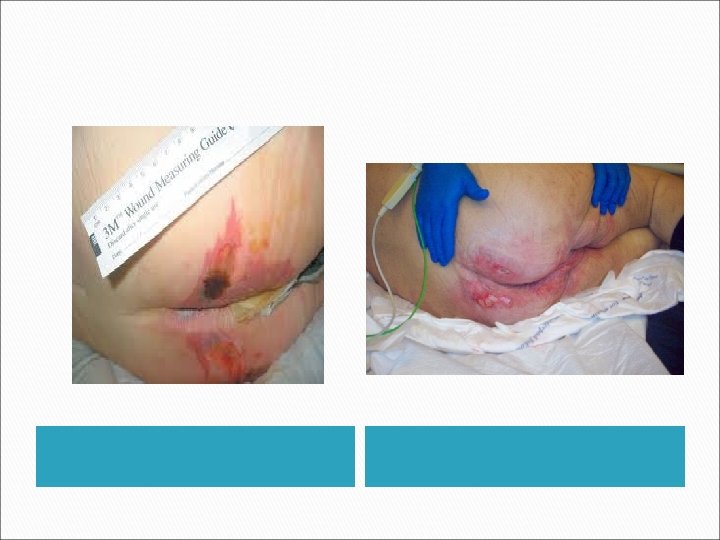
Deep tissue injury Purple or maroon localized area of discolored intact skin or blood filled blister due to damage of underlying soft tissue from pressure or shear. Area may be preceeded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue. Evolution may appear as a thin blister over a dark wound bed, may progress to eschar and further opening. Depth unknown. May or may not be reverseable. Keypoint: must monitor carefully. Use NONadhesive dressings to protect.
Deep Tissue Injury
Mucous membrane ulcers: don’t stage; describe what you see
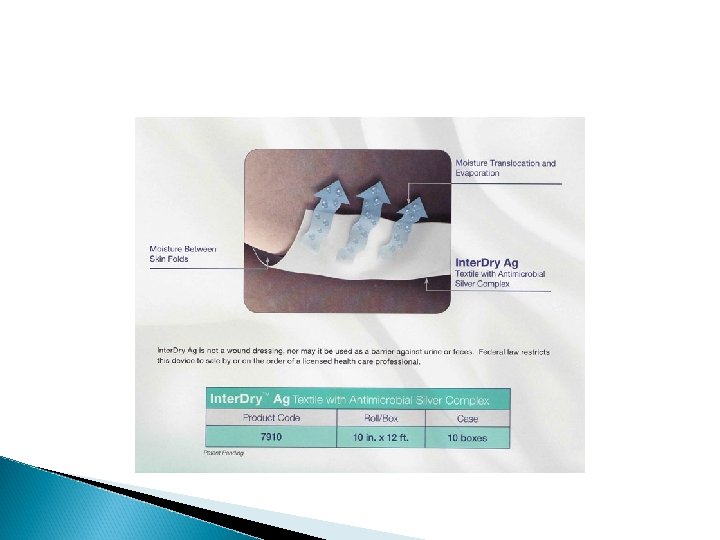
Intertrigo An inflammatory condition of the skin with our without skin loss in skin folds induced or aggravated by mechanical friction, maceration, moisture, heat. May have bacterial or fungal component. Often found in skin folds, axilla, gluteal fold, perineal area, abdominal panus, under heavy breasts. Morbidly obese high risk in skin folds.
Intertrigo with fungal infection
DOCUMENTATION PADB: Chronic skin issues? ? ? YES!! Further elaboration should be in note and on skin assessment Basic skin condition: moist, dry, flakey, skin turgor, ecchymotic, paper thin skin If wounds found on admit, ASK the pt. how, where, when acquired and DOCUMENT
DOCUMENTATION: WOUND CHARACTERISTICS MUST include: location, type of wound, color or general appearance of wound base (pink, red, slough, eschar, etc. ) Describe surrounding skin (intact, macerated, red, hard, moist, etc) Measurements: on finding wound and weekly Drainage (amount, character, color, odor or lack of odor) PAIN!! Presence or absence
DOCUMENT YOUR INTERVENTIONS ◦ Treatment done or condition of dressing if not changed ◦ Who notified ◦ Pain level/analgesia offered or given/response ◦ Pressure Ulcer prevention interventions/consults (WOCN, PT, OT, nutrition, turning, pressure offloading, specialty boots, specialty mattresses, Geomatt) ◦ Document education done with patient and family
CARE PLAN Patient/individual specific (difficult with EPIC) Measureable outcomes/Realistic Interventions: specific for patient vs. canned responses Special attention to Braden Scale using subscales with low scores : address in care plan interventions Document who was notified if unusual findings EVALUATE: is the treatment working? ? If not, what should you change? Address!
Current Treatment Specific Standards you can implement NOW Incontinence: Baby wipes, skin cleanser, skin barriers, moisturize with lotion, fecal pouches Offload pressure: Prevalon boots, pillows for bridging and turning, turning schedule, Geomatt cushion for sitting Resource utilization: WOCN, MD, CNS/Educator, Skin Champion
Nursing Interventions: No orders required: Stage I Options: open to air, dry dressings, Tegaderm, Allevyn, Alleyn Non-adhesive, skin prep Stage II: Allevyn, Allevyn non-adhesive, Tegaderm, use of Solosite Gel if wound bed dry in addition to cover dressing Deep. Tissue Injuries: Open to air (dry, non blistered); Allevyn NON-adhesive if blistered or thin skin coating and at risk with adhesives, Elastogel
Skin Tears: Superficial Xeroform or Vaseline gauze/Kerlix. AVOID adhesives. Change every 1 -2 days depending on drainage. Deeper tears or flap tears: extensive tissue damage and need MD or WOCN consult
Wound Wednesdays Wounds that have dressing orders should be measured, photographed and documented weekly; Wednesdays preferred. Fill out EPIC wound documentation, upload photo. You may document below photo or in care plan notes. Notify MD of findings, can click “cosign” to alert to photo
Are you an expert yet? ? ?
THE END!!