The Liver in Sickle Cell Disease Cage S


 Hepatitis: viral, drug-induced,")

























- Slides: 34
The Liver in Sickle Cell Disease Cage S. Johnson, M. D. Professor Emeritus of Medicine and of Physiology and Biophysics Director, Comprehensive Sickle Cell Center Keck School of Medicine, University of Southern California, Los Angeles, California, USA
Hepato. Biliary Complications • • • hemolysis & accelerated bilirubin catabolism Transfusion therapy Vaso-occlusion Disorders unrelated to the hemoglobinopathy SS> SC> S-thalassemias
Hepato. Biliary Complications: • • • Hepatomegaly Hepatic ‘crisis’ (RUQ syndrome) Hepatitis: viral, drug-induced, auto-immune Hemosiderosis Cholestasis: benign, progressive, drug-induced Hepatic sequestration Cirrhosis Inspissated bile/Choledocholithiasis Wide differential diagnosis
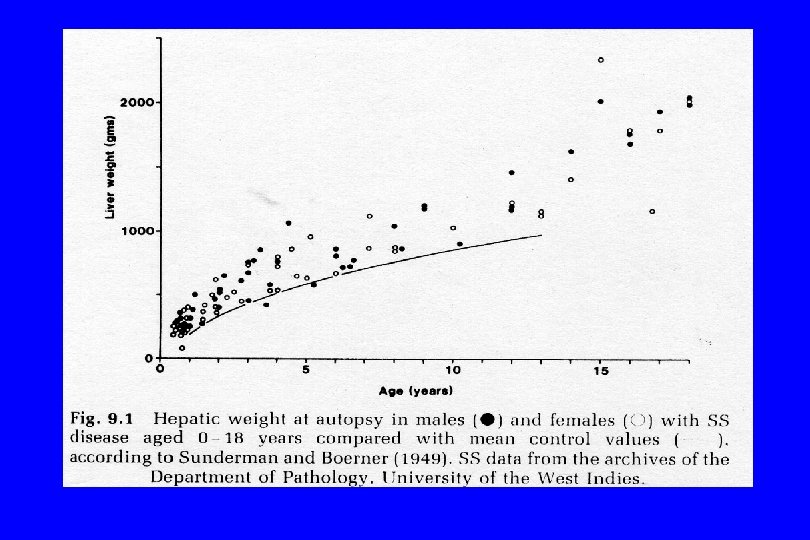
Hepatomegaly • Increased blood volume and blood flow • Hepatocyte hyperplasia • Kupffer cell erythrophagocytosis, sinusoidal distention • Extra-medullary hematopoiesis • Passive congestion in right heart failure (pulmonary hypertension Haematologia 22: 169, 1989 Serjeant, 2001 Am J Med 69: 833, 1980 Dig Dis Sci 31: 247, 1986 J Pediatr Hematol Oncol 24: 125, 2002
RUQ Syndrome • RUQ pain, leucocytosis – fever, nausea, vomiting • • Jaundice: 3 to 12 mg/d. L Variable elevation of AP & ALT Lasting 2 days to 3 weeks Differentiate from cholecytitis Amer J Clin Pathol 44: 1, 1965
Cent Afr J Med 40: 342, 1994 J Trop Pediatr 34: 59, 1988
Unusual causes of RUQ pain & abnl liver tests in Sickle Cell Disorders • • • Biloma Focal nodular hyperplasia of the liver in children Fungal ball Hepatic artery stenosis Hepatic infarct/abscess Hepatic vein thrombosis Mesenteric/colonic ischemia Pancreatitis Peri-colonic abscess Pulmonary infarct/abscess Renal vein thrombosis
RUQ syndrome • Abdominal Examination • Ultrasound • Biliary scintigraphy: high false positive rate [fasting, hepatocellular disease, chronic cholecystitis, extra-hepatic obstruction, narcotic-induced spasm of the sphincter of Oddi] low positive predictive value but high negative predictive value-patent cystic duct
Acute Viral Hepatitis N = 65: Hb SS - 6, Hb AS - 10, Hb AA (anemic) - 24, Hb AA - 25 • Peak bilirubin in Hb SS 4 x others; 40 mg/d. L vs. 12 mg/d. L • Hb SS 41 d vs. 25 to 38 d • AST, Alk P’tase, PT - no difference • Globulin persistently elevated in Hb SS • Degree of sickling on biopsy did not correlate with liver enzymes
Hepatology 19: 1513, 1994
The Liver in Sickle Cell Disease Hb SS, n=100: Hb SC, n =25: 78 elev. Ind. Bili only 22 elev. Ind. Bili only Hb SS Hb SC HBs. Ag + 3 1 HCV + 64 11 CLD 13 3 Ind. Bili 6 Medicine (Balt) 64: 349, 1985 Dig Dis Sci 31: 247, 1986
Auto-immune Hepatitis • Painless jaundice & marked poly-clonal gammopathy • Positive ANA, SMA, LKM-1 or SLA/LP • Histology shows dense T-cell peri-potal infiltrates • Extra hepatic manifestions: arthropahty, rash, leg ulcers • Rx: prednisone/azathiprine for 24 months Haematolgia 19: 49, 1986 Am J Gastroenterol 91: 1016, 1996 J Pediatr Hematol Oncol 19: 159, 1997
Chronic Liver Diseases Hb SS, n =22: Cirrhosis with hemosiderosis - 5, Cirrhosis without hemosiderosis, Chronic active hepatitis B - 2, Druginduced cholestasis - 2, chronic passive chogestion, and 1 each with elev. Alkaline phosphatase - bone, common duct obstruction, Histiocytic lymphoma, sarcoidosis, benign cholestasis of pregnancy, acute viral hepatitis B and five unexplained. Hb SC, n = 3: 1 each with Alcoholic Liver Disease, granulomatous Hepatitis, unexplained. Medicine (Balt) 64: 349, 1985 Dig Dis Sci 31: 247, 1986
Predictors of Liver disease Alb < 3. 2 g/d. L Glo > 4. 0 g/d. L Bili t > 4. 0 mg/d. L Bili d > 0. 5 mg/d. L Alk Ptase > 225 IU ALT > 100 IU ALT > 50 IU AST > 100 IU AST > 50 IU Ferritin > 500 ng/m. L Ferritin > 300 ng/m. L X 2 P< 2. 2 5. 9 28 8 51 7 22 21 16 9 10 . 08. 05. 0001. 015. 0001. 0002. 01. 01
Liver Histology n= Sickling Ischemc necrosis Viral hepatitis Miscellaneous Other Disease NSL Biopsy 19 17 1 8 2 2 5 Autopsy 32 30 14 3 4 1 10 Dig Dis Sci 31: 247, 1986
Hepatic Sequestration • Occurs about 1 per 161 admissions • Progressive enlargement of the liver with falling hemoglobin rising reticulocyte count • Markedly elevated bilirubin, predominantly conjugated fraction • Alkaline phosphatase as high as 650 IU • Modest elevation of transaminases [< 110 IU] • Obstruction of flow by vso-occlusion in small hepatic veins and/or sinusoids • Rx: exchange transfusion preferred BMJ 294: 1206, 1987 BMJ 290: 744 & 1214, 1985 Postgrad Med J 72: 487, 1996
Postgrad Med J 72: 487, 1996
Am J Hematol 42: 81, 1993
Br J Haematol 89: 757, 1995
Blood 96: 76, 2000
Blood 96: 76, 2000
Cirrhosis • • Hepatitis B or C, auto-immune Hemochromatosis Chronic passive congestion Miscellaneous: alcohol, toxins, sarcoidosis, cryptogenic, chronic biliary obstruction
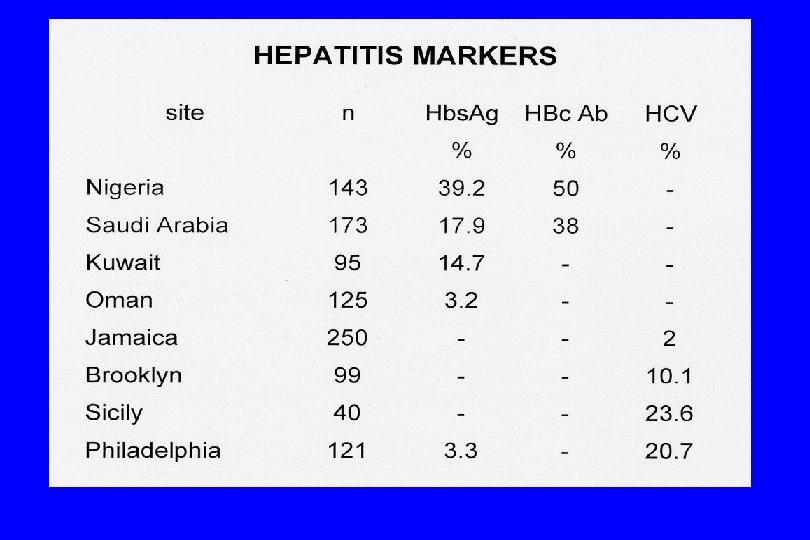
Summary 1. The majority of patients have only elevations of indirect bilirubin and LDH due to hemolysis 2. Chronic abnormalities in liver function are due to a wide variety of disorders other than the hemoglobinopathy. Judicious use of liver biopsy is often required for specific diagnosis. 3. Evidence for hepatitis B and C infection is common. Patients seropositive for hepatitis C have significantly greater serum globulin and transaminase levels than those seronegative.
Summary 4. Kuppfer cell erythrophagocytosis and intrasinusoidal sickling are universally found in hepatic histology and are not related to the degree of transaminase elevation. The absence of shrunken hepatocytes speaks against the concept of anoxic liver damage and is more consistent with the liver as the site of RBC destruction in the absence of splenic function. 5. The increasing use of transfusion therapy in this patient population is associated with a high frequency of trnasfusion transmitted viral disease and iron overload; prudence dictates ongoing surveillance for these and other liver disorders that may affect these patients.
Br Med J 295: 234, 1987
N Engl J Med 307: 798, 1982
J Pediatr 136: 80, 2000
Gastroenterology 112: 463, 1997