Stuttering Part 3 a CHAPTER 4 ASSESSMENT ADOLESCENTS








")

 usually translates to duration Muscular tension throughout body before")











 � Self-Efficacy Scale for Adult Stutterers (SESAS) Figure 4")







 study. 45 children being assessed for stuttering")



 • Head and eye movements (Conture and Kelly, 1991) •")




")
 • A strong family history")
")
 • Speech Situation Checklist—Emotional Reaction")
- Slides: 47
Stuttering Part 3 a CHAPTER 4 ASSESSMENT: ADOLESCENTS & ADULTS DOUGLAS B. PETERSEN, PH. D. , CCC-SLP SPPA 5120
Help Me to Speak part 4 � https: //www. youtube. com/watch? v=W_16 Z 6 gz. IZQ �
Surface and Intrinsic Features �Surface Frequency Duration Tension Dramatic accessory features �Identifying the quantity and quality of surface features provide one indication of severity and provide a means of progress monitoring.
Surface and Intrinsic Features �Instrinsic Surface behaviors can inform the nature of what is happening under the surface. Motivation for change � Statements made by the client do not always reflect true level of motivation (I’m going to run 3 miles every day). � It is, in the end, the speaker’s motivation and determination that determine how quickly they will change.
Surface and Intrinsic Features �Assess Motivation � Describe the treatment steps and the process � Ask how much treatment is worth to them � How far would they be willing to drive � Why are you here today and not 6 months ago?
The Initial Meeting �Convey: You are not alone You can improve your fluency You can improve your life �Remember? Hope? Love? YOU? Again, the clinician is probably the most important element. You are the guide, the coach, the motivator.
Two Principles of Assessment � 1. To what degree is the person using open decision making about communicating? Assess how much stuttering alters the person’s choices and options in life. � What do you do because you stutter? � 2. To what degree is the person attempting to speak with an open and flexible vocal tract? Assess the level of struggle and effort. � What does the speaker do when he or she stutters?
A Note On Severity �Severity is not judged simply by observing outward stuttering events. �Frequency and form are not the prime indicators of severity, it is the person’s response that dictates severity. Some people who would otherwise be considered a person who stutters severely (based on outward behavior) may be affected very little by their stuttering, and visa-versa. �Severity = Distress X Uncontrollability X Frequency
Mapping Surface Features �FREQUENCY �TENSION �DURATION �DRAMATIC BEHAVIOR (ACCESSORY FEATURES)
Frequency �Frequency of fluency breaks Calculate the percent of stuttered syllables or stuttered words. Syllables are the preferred unit of analysis. �During conversation �While reading
Tension and Duration �Tension (effort) usually translates to duration Muscular tension throughout body before or during stuttering event. High levels of tension = tremors. � Lips � Tongue � Velum Fragmentation (part-word repetitions) � Initiation of a word or syntactic unit Blocks � Vocal tract is occluded and airflow and voicing stop. � Closure usually occurs at vocal folds – but plosives also contribute. � Don’t just note the occurrence. Ask yourself HOW it is being done.
Prominent Behaviors �Verbal and physical movements Prior to During
Subtle Surface Features �Avoidance People Sounds Words Time pressure Environments � It is natural to do, but an unproductive strategy � It reduces participation in life � It reduces choices Sometimes you just need to give people permission to stutter.
Subtle Surface Features �Substitution A feared word is replaced �Postponement A moment of hesitation � Slight pause � A filler word/phrase (um, uh, you know, let me see)
How Does the Client Assess Him-/Herself? �Scale of 0 -8 0 = no stuttering 1 = mild stuttering 8 = severe stuttering �Have the client indicate what their overall stuttering is like. �Mark an ‘A’ for average above the number indicated. �Have the client indicate what their stuttering is like right now. �Ask the client how much their stuttering varies.
Therapy Trials �Have the client stutter with you. Purposeful stuttering Brings the client under control. They are in charge of their stuttering. �The ability to employ purposeful stuttering reflects Clients level of anxiety Clients motivation
Intrinsic Features �What do you do because you stutter? �What do you not do because of the possibility of stuttering? �Identifying loss of control The clinician should express understanding of what it feels like to be out of control. Calibrate yourself to your client. Recognize and verify the occurrence of losing control.
Cognitive and Affective Factors � Helplessness � Fear � Shame � Avoidance � Blame � It has been proposed that “the clinician is the major agent for assisting clients to transform the meaning of their stuttering, which in turn, will provide both a reduction in suffering and facilitate the modification of overt behaviors. ” � Get the client’s story.
Assess The Speaker’s Decision Making �Help the client identify and acknowledge that they do make choices to avoid stuttering. �Decrease avoidance behaviors (Increase stuttering – this is OK, and can be perceived as a sign of progress!)
What is stuttering? : Some criteria for diagnosis � 3 or more sound/syllable repetitions ([I-I-]I), and/or prolongations ([wwww]we) per 100 syllables of speech. � Clustering of sound/syllable repetitions and/or prolongations (e. g. , [They]They [ha-]have to go). � Majority of disfluencies are sound/syllable repetitions and prolongations. � Mean # of iterations per repetition > 1. 5 (e. g, [h-h-he]). � Average duration of repetitions and/or prolongations exceeds that of nonstutterers (e. g. , > 0. 75 seconds). � Tempo of repetitions is “rapid” or “irregular. ” • (Gillam 2010)
What is stuttering? Some additional considerations �Atypical physical tension, struggle, or bodily movements during fluent or disfluent speech. �Negative feelings related to speech (e. g. , frustration, fear, embarrassment, shame). �Maladaptive compensatory strategies word substitution situational avoidance • (Gillam 2010)
Some formal assessment measures • Equal-Interval Scale Figure 4 -1 • Locus of Control of Behavior (LCB) Figure 4 -2 • Stuttering Severity Instrument (SSI-4) Figure 4 -3 • Subjective Screening of Stuttering Severity (SSS) Figure 4 -4 • Revised Communication Attitude Inventory (S 24) Figure 4 - 5 • Perceptions of Stuttering Inventory (PSI)
Some formal assessment measures (continued) � Self-Efficacy Scale for Adult Stutterers (SESAS) Figure 4 -6 � Self-Efficacy for Adolescent Scale (SEA-Scale) � Figure 4 -7 � Overall Assessment of the Speaker’s Experience of � Stuttering (OASES) [The Speaker's Self- Assessment] Figure 4 -8 � Wright & Ayre Stuttering Self-Rating Profile (WASSP) Figure 4 -9
Practice Transcribing/Coding � SSI-3 Practice Session 1 � Woman from HCRI: http: //www. youtube. com/watch? v=tank 0 i. W 1 q. OA&feature=related Listen to and watch video/Transcribe Identify Syllables (dot above each syllable) Identify Disfluencies (slash through stuttered syllable/identify disfluency) As a class complete the SSI-4 Record Form (on overhead) � SSI Practice Session 2 (Independent) � Joel Korte: http: //www. youtube. com/watch? v=ATp. W_On. C 308&feature=related Watch Joel Korte video and check transcription (handout) Identify Syllables Identify Disfluencies Complete SSI-4 Record Form (handout) � Criterion Referenced Assessment Session Joel Korte Video Follow procedures for criterion referenced assessment (handouts) On Overhead
Stuttering Part 3 b ASSESSING YOUNG CHILDREN
The First Meeting with Parents • Demistify the phenomenon—stuttering is not a bad word • Decrease guilt and shame—it’s nobody’s fault • Explain onset and development • Inform about the future of their child • Explain the treatment process • What they can do • Get a case history • 42% chance someone in the nuclear family stutters • 71% chance someone in the extended family stutters • Academic Performance • Self-Esteem • Psychosocial Functioning • Family Structure/History
The First Meeting with Parents • We can learn: • The rules and regulations in the child’s life. • The parents attitudes toward child rearing. • Pertinent issues within the parental relationship • Problem solving strategies employed • The place the disfluency problem holds within the family • Start interview with general concepts then move toward more sensitive and emotional material • Caruso (1988)
Assessment: Two Basic Decisions for Children � 1. Is the child stuttering? We are good at identifying stuttering-like-disfluencies. � 2. Is it temporary? We have difficulty predicting recovery. Yari and Ambrose (2005) say about 85% of children spontaneously recover (completely).
Most Children Recover • Incidence about 4– 5% • Prevalence about 0. 5– 1. 0% • Onset usually at 2– 4 years (mean of 33 m. ) • Recovery rate @ 75%– 85% by age 6 • Remission especially high first 6 months
1. Is The Child Stuttering? �Variability is considerable with young children. Good news: variable behavior is easier to change. Bad news: variable behavior is difficult to measure. �Obtain 300 -500 word sample Produced in a variety of natural settings Can attempt to obtain a representative sample in the clinic setting HOWEVER…
Variability! �Keep in mind the Yaruss (1997) study. 45 children being assessed for stuttering Tested in 5 different contexts � Parent-Child Interaction � Play with Pressures Impossed � Story Retell � Picture Description 19 of the children had fewer than 3% disfluencies in at least one context. 18 of those same children produced more than 10% difluencies in a different context.
Eliciting Disfluency �Place temporary demands on the child’s speech Turn away as the child is describing an event Ask the child to name pictures as quickly as possible Talk over the child Ask the child to respond to a series of questions that are complex Ask the child to read a book that is at a relatively high level Ask the child to describe pictures at a fast rate Bring other listeners into the room to distract or interrupt �It is not necessary to elicit a large number of fluency breaks �Consult with the parents to make sure your sample is representative
Is The Child Stuttering? �If there are two or more of the following…treatment is recommended The frequency of disfluencies are greater than 10% Sound prolongations make up more than 30% of within-word disfluencies Score of 19 or greater on the Stuttering Severity Instrument Score of 17 or greater on the Stuttering Prediction Instrument Stuttering is accompanied by eye movements to the side and/or blinking Clusters of stuttering constitute 25% of disfluencies Child has been stuttering for 18 months or more
Is The Child Aware? Is there Anxiety? • No clear differences in anxiety at outset (NFC v CWS); anxiety tends to increase over time (Yairi & Ambrose, 2005) • Puppet Study (Ambrose & Yairi, 1994) • CWS identified with the puppets that stuttered • Temperament • More sensitive, inhibited, and reactive • Inhibited with strangers, low tolerance for disfluency • Fertile ground where stuttering will grow? • A contribution to or a consequence of stuttering? • Some of these features ARE present at birth
Awareness and Anxiety (continued) • Head and eye movements (Conture and Kelly, 1991) • Pitch rise, schwa substitutions, fear, avoidance behaviors, decreased speaking—electively mute • Results with Kiddy. CAT (Vanryckeghem, Brutten, & Behavior Assessment Battery (BAB) • Herandez, 2005; CWS = 4. 36 v. NFC − 1. 79 (negative self-report scores) • Using projective drawings (De. Vore, Nandur, & Manning, 1984) • smaller drawings, lower-left quadrant pre-tx
Educational Impact �In the school setting the disfluency must have an adverse academic impact in order for the child to receive services. Refuse to participate in class discussions Avoid oral presentations Won’t respond to questions Pretend not to know the answer Pretend they are sick when presentations are required Social penalties See Table 5 -2 (Manning, 2010, p. 253)
Summary of Stuttering Signs • Occurrence of stuttering in nuclear or extended family * • Parents identify child as stuttering • SLDs increase when communicating under pressure • SLDs accompanied by tense movements of head, face, & neck • Behavioral or formal indicators of negative psychosocial reactions to stuttering • The child self-restricts communication and social interaction • The child is easily upset by changes in routine or inhibited with strangers
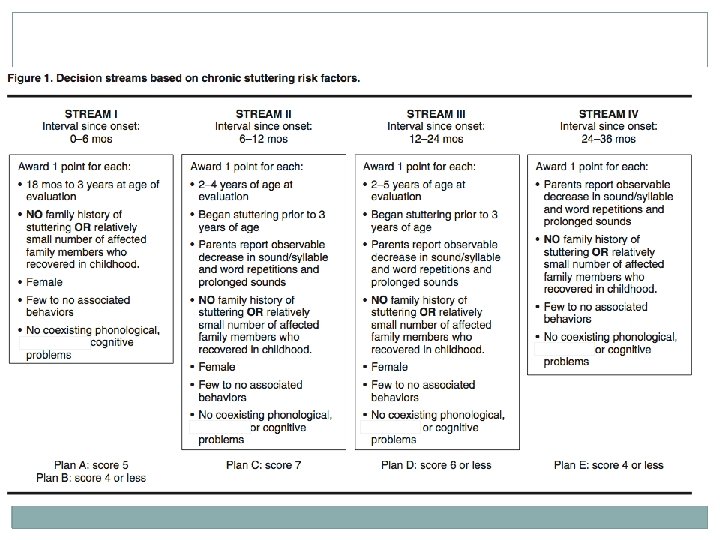
Children likely to become fluent: Green flags • Female • Less than three years old • Few relatives who stuttered • Relatives who did, recovered • May be severe at onset • Rapid decrease in severity • Fewer stuttering-like disfluencies (SLDs) • Normal expressive language
Children likely to be chronic Red flags • Male • Family history of persistence • Little or no decrease in weighted SLD by 12 months post onset • Phonological skills decrease after onset • 2– 3 times more SLDs: • • • Children Who Stutter (CWS): SLD = 66% Normally Fluency Children (NFC): SLD = 28% Clustering of fluency breaks 2+ part-word repetitions Faster repetitions More head & eye movements
Yairi & Ambrose (2005)
The best estimates of chronicity? (Yairi & Ambrose, 2005) • A strong family history is the single most reliable predictor of persistence and remission • Boys > girls • Decrease in SLDs first year following onset • A flat or inclining function suggests chronicity • Onset later than typical 33 months • Longer strings of part-word repetitions
Table 5 -2 Yairi & Ambrose (2005)
Procedures for assessing children • Behavior Assessment Battery (BAB) • Speech Situation Checklist—Emotional Reaction (SSC-ER) • Communication Attitude Test (CAT) • Speech Situation Checklist—Speech Disruption (SSC-SD) • Behavior Checklist (BCL) • Kiddy. CAT • Responsibilities of the IEP team (Ramig and Dodge, 2005) • TOCS