STARTER DATA ANALYSIS Read Data Sheet Complete Questions








 Some drug companies sell")










")



- Slides: 27
STARTER - DATA ANALYSIS • Read Data Sheet. • Complete Questions • Identify and explain three differences in healthcare between MEDCs & LEDCS (9 marks)
History of Health: European diseases spreading to the Global South
History of Health: Traditional Medicine vs Scientific Medicine
History of disease Many of the diseases seen in the developing world currently were faced by the developed world. There are some diseases that threaten to return to Europe. There are 3 things which controlled the diseases; • Improvements in nutrition and diet • Improvements in hygiene- clean water/sewage disposal • Changes in reproductive behaviour- falling birth rate These factors were also helped by education. • The western model of medicine has been forced onto developing nations during the colonial period, western hospitals are often costly, with unreliable modern technology and in cities not rural areas. Doctors who are trained in this system have no incentive to work and often only work for the 'urban elites', or leave the country (brain drain). Two options for developing nations • Selective biomedical intervention; mass vaccination programmes, vitamin supplements or insecticide nets. This can lead to reduction in child mortality but is not sustainable, preventing one disease now might not rule out another later one. • Comprehensive primary healthcare; community based with an emphasis on healthcare education and prevention of disease – e. g. draining ponds so mosquito cannot breed, contraception training, basic first aid training.
Requirements for improved Third World Health. Patterns of third world health Health and Development Problems of measuring health Wealth V Health Third world health and the developed world
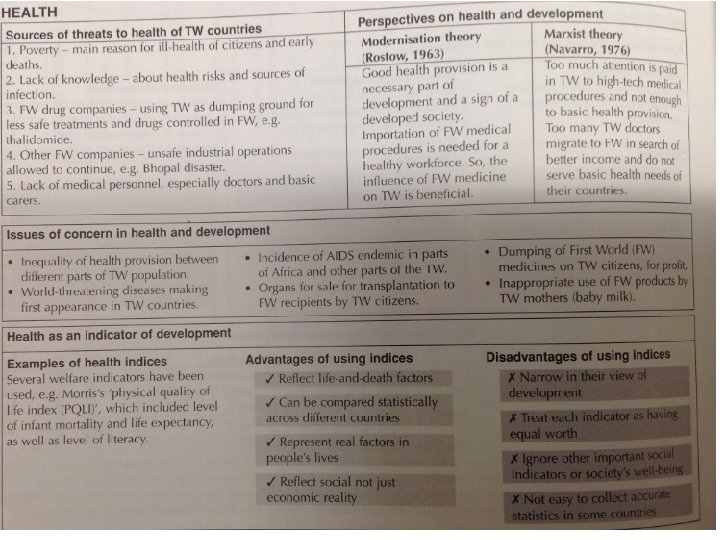
Problems of Measuring Health • Recording statistics e. g. The PQLI (physical quality of life Index) measure infant mortality, literacy and life expectancy. The PSQLI allows sociologists to compare trends across countriess. Validity • PQLI is a limited measure of basic needs • Many societal and psychological factors like security, justice, human rights, etc are excluded. • Does not explain the changing structure of economics and societal development. • Arbitrary weights are given to each determining factors. • PQLI does not measure economic development and total welfare. PQLI is a limited measure of basic needs Global Progress * Fall in Death Rates and IMR * Increase in Life Expectancy
Wealth vs Health Are wealth and health inter-related? * Positive correlation between GNP and level of health * Differences exist between countries in same GNP band * Generally disease thrives in environment of poverty * Millions live in downward spiral of poverty and are prone to disease, ill health, unemployment and further poverty
Patterns of Third World Health Access to medicines- (External Barrier) Some drug companies sell drugs in the developing world that are banned in the west for safety reasons. Or they may set the price of drugs so high that many can’t afford them. E. g. HIV AIDS drugs. Until 2001 TNC drug companies refused to allow local drug companies to make cheap versions of anti-HIV drugs. Health and Education- (Internal Barriers) The lack of good health education in the developing world means many people (particularly those in traditional rural areas) do not know how to prevent disease and are not aware of basic treatment. Universal health care is rare in the developing world- people usually have to pay to see a doctor. There are not enough doctors and nurses to go around.
Third World Health and the Developed World * Imperialism brought disease and death * Replacement of nutritional crops for cash crops reduced health of local populations and lead to food crisis * TNC’s research/test new pesticides and drugs in developing countries often with harmful effects * Location of manufacturing plants with limited concern for pollution and environmental effects * Marketing of certain foods and drinks i. e. cola/chocolates and tobacco have led to harmful effects * Health care modelled on the West is centred in urban areas and is very technical based and expensive – not catering for the majority of the population * Emphasis on “curative” rather than “preventative “medicine
Requirements for improved Third World Health Need for: • Water and sanitation • Nourishment • Literacy and sexual equality • Primary health care
However… Africa still faces high rates of disease, disability, and death. *Average life expectancy is 47 years. * Health systems in Africa are weak in part because of poverty, communicable and non-communicable diseases, and a shortage of health-care workers. * Many people do not have access to health care. * Approximately 800 African children continue to die everyday because their parents cannot afford to pay for medical services. Millennium Development Goals (MDGs) were set to reduce health problems by 2015 Mothers bring their children in for a periodic check at the Reproductive and Child Health (RHC) clinic in Tanzania
At the UN-sponsored Millennium Summit in 2000, the world’s nations unanimously made a commitment to reach eight targeted goals, now known as the Millennium Development Goals (MDGs), by the deadline of 2015. Some success but targets not met. Student Task: What are the new Health Targets on the SDGs?
STARTER Word Fill Reflection Answers 1. 2. 3. 4. 5. 6. Poverty forces people to suffer a bad diet and poor public health. It also prevents them from gaining a good quality of health care. Universal free health care is rare in the developing world – people usually have to pay to see a doctor. There also not enough doctors and nurses to go around. The lack of good health education in the developing world means many people (particularly those in traditional, rural areas) do not know how to prevent disease and are not aware of basic treatments. Some drugs companies sell drugs in the developing world that are banned in the West for safety reasons. Or they may set the price of life-saving drugs so high that many people in LEDCs can’t afford them. Western products may be used inappropriately. For example, baby formula milk is heavily advertised in LEDCs. But some mothers don’t have access to clean water to make the milk with, so many babies die from infections. And poor mothers may water down the formula too much (to make it last longer), resulting in malnutrition. Also, TNCs that have set up in developing countries often pay little attention to the environment, or health and safety. For example, the Bhopal poison gas leak of 1984 happened because safety procedures were inadequate. For example: HIV/AIDS in South Africa • • Insufficient health education in poor areas meant people didn’t know how HIV was transmitted. Clinics could be a day’s walk away Transnational drugs companies refused to allow local drugs companies to make cheap versions of anti-HIV drugs. This practise was banned by the courts in 2001 In the 1990 s, the South African government was reluctant to distribute anti HIV drugs as they doubted that HIV caused AIDS.
Theoretical views about health inequalities MODERNISATION THEORY • Modernisation theorists and functionalists believe Western medicine is superior, and that Western medicine and health education can solve the problems of high infant mortality and low life expectancy. Rostow (1971) (5 stages of modernisation) said high-tech medicine used in the developed world should be transferred to developing nations so that quality health care can be provided. However, these countries my lack the relevant infrastructure, and or aid/trade to afford these high-tech medicine. • The developing nations are where the developed world were hundreds of years ago, and Modernisation theorists expect them to follow the western path. We are now in Epidemiologic transition which is a change from infectious diseases, resulting in high child mortality and low life expectancy to ' diseases of affluence' where the highest killers are heart disease and cancers. Developing nations should drop traditional medicines, opt for a centralised healthcare system based on doctors and mass immunisation. They should look at aid and expertise from the developed word. DEPENDENCY THEORY • Marxists: Navarro (1976) believed that high-tech Western health care is not the immediate priority for the developing world. Poor nations need to focus on basic health procedures to save lives and improve quality of life. Doctors from these nations need to be encouraged to stay and work in their won countries, not to migrate to MEDCs for better pay (“the brain drain”). • Dependency theory blames colonialism and exploitation. Colonialism introduced European diseases to Africa, America and Asia, e. g. Smallpox from Spain to South America. Colonialism also replaced nutritional food crops with cash crops, resulting in malnutrition. Dependency theory also blames the developed world for poverty and debt leading to an inability to invest in healthcare. Developing countries can't be expected to follow the west, colonialism changed health and neo- colonialism continues this trend. There are factors affecting health in these countries; • adopting lifestyles of the rich world (sugary/fatty)can lead to cancers and heart conditions • power of TNC's to advertise sugary/fatty foods irresponsibly and avoid attempts to restrict them • pollution and environmental damage caused by TNC's affect health • TNC's are reluctant to sell medicine at affordable prices/let them manufacture their own • poor funding for medicine and treatments that would help those in the south, now they are targeted at weight loss and cosmetics • structural readjustment programmes give little scope for states to improve health care, charges have to be made and poor can't afford it.
Theoretical views about health inequalities • Neoliberals believe in a privatised health care service, and a bare minimum laid out by the sate. TNCs should be free to develop drugs and medicines that are cost effective. With pharmaceutical companies competing to discover and create new drugs and medicines it will drive the price down for consumers / governments. Structural Adjustment Programmes need to be put into place to ensure this transition. However, this could lead to poor quality (cheap & basic healthcare provision), a class division of those that can afford and those that can’t, and TNCs / governments unwilling to invest in products that aren’t cost effective, leading to deaths of certain sufferers. • Counter Industrial Theorists would advocate a people centred approach, focussing on specific needs on certain communities, rather than a topdown whole country approach, e. g. only certain regions may be prone to chloera. They would also support micro financing local communities to setup a effective long term health system, rather than investing in nationwide ‘mega-hospitals’.
RECAP: Steve Bassett • https: //www. youtube. com/watch? v=ax. Mh 1 uz 77 b 8&index=19&list=PL 416 u 5 b. H 2 h 7 FBsdybjo Gtr. Dy. ZHEXEZAn 5 • Homework: Further Notes from Textbook
Homework Practice Question (18 marks)
Essay Plan • Developing World & Healthcare. • Barriers to Healthcare in Developing World. • Theoretical viewpoints in relation to the question.
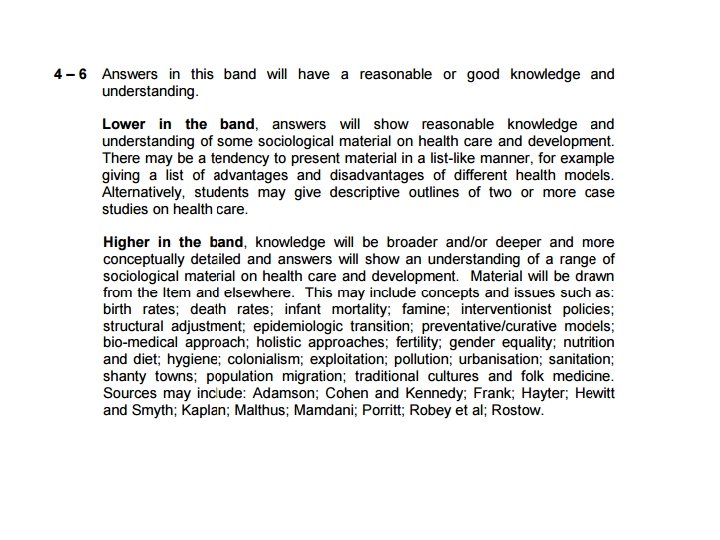
TARGETS T 1 – Link in Theory that you have not covered (Modernisation, Dependency, Neoliberal, Counter-Industrial/Post-development) T 2 - Include any of the concepts you have not included from the mark scheme (Slide 23 of Power. Point ). T 3 – Discuss barriers to healthcare and healthcare improvement in the developing world, and link to the question. T 4 – Link in all of these key areas: epidemiological transition, prevantative vs curative strategies, traditional cultures and folk medicine vs modern cultures and scientific medicine. T 5 – Refer to the history of medicine in your introduction. T 6 – Add regular links to you writing that show you are answering the question (e. g. this shows that Western Models/Practices are / are not appropriate for development). T 7 – Refer to at least 3 Sociologists in your answer (check the Textbook, Mark Scheme & your notes and make sure you use them in your answer). T 8 – In your conclusion, give an overall judgement, including the most positive and negative arguments to support / discredit the statement in the question. T 9 – Link in MDGs / SDGs
June 2017