Spondylolisthesis Presenter Ang Mu Liang Moderator Mr Aravind







 Classification of spondylolisthesis as a guideline for")









 • Physiotherapy – Lower abdominal – Hamstring stretch")


 • Uninstrumented")












 of surgical management of degenerative")




- Slides: 43
Spondylolisthesis Presenter: Ang Mu Liang Moderator: Mr Aravind
Contents • • Types of spondylolisthesis Severity Radiological parameters Spondylolisthesis – Adult Isthmic – Degenerative
Definition • Spondylolysis – Defect in the pars interarticularis • Spondylolisthesis – Forward slippage of one vertebra on another
Spondylolisthesis Severity • Meyerding Grades I to V – The grade of spondylolisthesis is determined by dividing the sacral body into four segments – Grade V as spondyloptosis.
Spondylolisthesis Classification 1. Newman, Wiltse and Mac. Nab 2. Marchetti and Bartolozzi 3. Spinal Deformity Study Group
Spondylolisthesis Classification • Newman, Wiltse, Mc. Nab Classification
Spondylolisthesis Classification • Newman, Wiltse, Mc. Nab Classification
Spondylolisthesis Classification Marchetti PC, Bartolozzi P (1997) Classification of spondylolisthesis as a guideline for treatment. In: Bridwell KH, De. Wald RL, Hammerberg KW, et al. , (eds) The textbook of spinal surgery, 2 edn. Lippincott-Raven, Philadelphia pp 1211– 1254
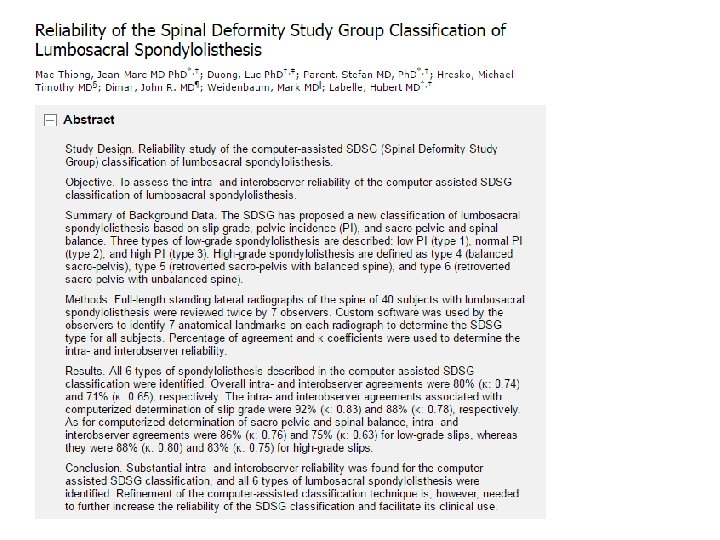
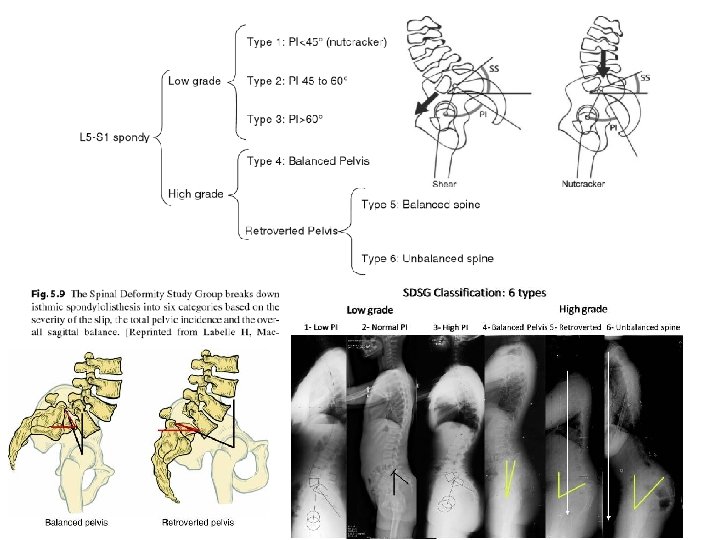
Spondylolisthesis Classification • Spinal Deformity Study Group – Based on • • Slip grade Pelvic incidence Sacro-pelvic balance Spinal balance – 7 anatomical landmarks – 6 types
Spondylolisthesis Severity Other Measurements Angles Remarks 1. Slip angle < 0 degrees Signifies L 5 -S 1 lordosis 2 a. Sacral inclination 2 b. Sacral slope 40 +/- 10 ( < 30 deg) 3. Pelvic incidence 50 +/- 10 4. Pelvic Tilt 15 +/- 5 5. α angle – L 5 incidence - Correlates with slips
Spondylolisthesis Severity Other Measurements Angles Remarks 1. Slip angle < 0 degrees Signifies L 5 -S 1 lordosis 2 a. Sacral inclination 2 b. Sacral slope 40 +/- 10 ( < 30 deg) 3. Pelvic incidence 50 +/- 10 4. Pelvic Tilt 15 +/- 5 5. α angle – L 5 incidence - Correlates with slips
Spondylolisthesis Severity Other Measurements Angles Remarks 1. Slip angle < 0 degrees Signifies L 5 -S 1 lordosis 2 a. Sacral inclination 2 b. Sacral slope 40 +/- 10 ( < 30 deg) 3. Pelvic incidence 50 +/- 10 4. Pelvic Tilt 15 +/- 5 5. α angle – L 5 incidence - PT SS Correlates with slips
Spondylolisthesis Severity Other Measurements Angles Remarks 1. Slip angle < 0 degrees Signifies L 5 -S 1 lordosis 2 a. Sacral inclination 2 b. Sacral slope 40 +/- 10 ( < 30 deg) 3. Pelvic incidence 50 +/- 10 4. Pelvic Tilt 15 +/- 5 5. α angle – L 5 incidence - Correlates with slips
Natural history • Unilateral pars defects almost never slip • Progression of spondylolisthesis slows over time • In adults – Radicular symptoms • Narrowing of neural foramen and compression of exiting L 5 root – 3 phases of degenerative spondylolisthesis (Kirkaldy-Willis) 1. Dysfunction 2. Instability 3. Restabilisation
Adult isthmic spondylolisthesis • Presentation – Low back pain – L 5 radicular pain • Etiology – Associated with an increased pelvic incidence • PI ↑, SS ↑, Lumbar lordosis ↑ to maintain sagittal balance – Normal pelvic incidence: 50 to 55 degrees – Patients with spondylolisthesis: 70 to 80 degrees. • PI does not predict progression of listhesis. – Pars defect – L 5 radiculopathy • L 5 -S 1 most common • Compression of exiting L 5 nerve root by fibrous repair tissue at the site of the defect.
Degnerative spondylolisthesis • Epidemiology – More common: diabetes and women older than age 40 – Most frequent at the L 4 -L 5 level – Reported more common: transitional (sacralized) L 5 vertebrae and sagittally oriented facet joints. • Presentation – L 5 radiculopathy from central and lateral recess stenosis • Root compression in the lateral recess between the hypertrophic and subluxated inferior facet of L 4 and the posterosuperior body of L 5
SPECT-CT • SPECT: highest sensitivity for bone activity • CT: highest anatomical specificity • Neg CT + Pos SPECT – Stress response, Pre-lysis – Good prognosis for healing and bony union • Pos CT + Neg SPECT – Non-union chronic lesion
Treatment • Activity modification • (Bracing) • Physiotherapy – Lower abdominal – Hamstring stretch – Spinal flexion • Pars blocks
Surgical indications • • Failure of conservative rx Progression of slip Presenting with 50% slip Neurological deficit/deformity Surgical goals • Decompression of neural elements • Stabilisation of spinal segments
Pars repair
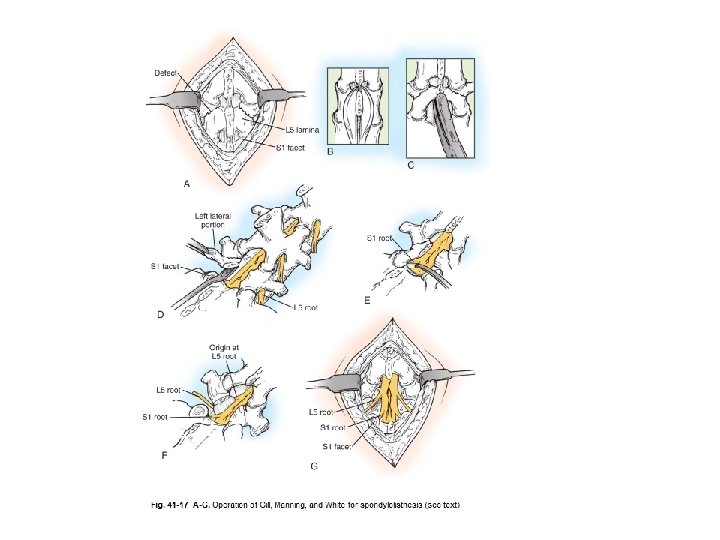
Surgery • Decompression – Without fusion: Gill’s procedure – With fusion (posterolateral) • Uninstrumented • Instrumented
Inter-body fusions • • Better reduction Restore foraminal height Bigger surface area for fusion Graft is under compression
ALIF v TLIF v PLIF v DLIF v XLIF v Axia. LIF v OLIF
Question #2: What is the natural history of degenerative lumbar spondylolisthesis? • Most of the patients with symptomatic degenerative lumbar spondylolisthesis and an absence of neurologic deficits will do well with conservative care. • Patients who present with sensory changes, muscle weakness, or cauda equina syndrome, are more likely to develop progressive functional decline without surgery. • Progression of slip correlates with jobs that require repetitive anterior flexion of the spine. • Slip progression is less likely to occur when the disc has lost over 80% of its native height and when intervertebral osteophytes have formed. • Progression of clinical symptoms does not correlate with progression of the slip.
Question #6: Do medical/interventional treatments improve outcomes in the treatment of degenerative lumbar spondylolisthesis compared with the natural history of the disease? Question #7: What is the role of pharmacologic treatment in the management of degenerative lumbar spondylolisthesis? Question #8: What is the role of physical therapy/ exercise in the treatment of degenerative lumbar spondylolisthesis? Question #9: What is the role of manipulation in the treatment of degenerative lumbar spondylolisthesis? Question #10: What is the role of epidural steroid injections for the treatment of degenerative lumbar spondylolisthesis? Question #11: What is the role of ancillary treatments, such as bracing, traction, electrical stimulation, and transcutaneous electrical stimulation in the treatment of degenerative lumbar spondylolisthesis? Question #12: What is the long-term result of medical/interventional management of degenerative lumbar spondylolisthesis? • A systematic review of the literature yielded no studies to adequately address any of the medical/interventional treatment questions posed above.
Question #13: Do surgical treatments improve outcomes in the treatment of degenerative lumbar spondylolisthesis compared with the natural history of the disease? • Surgery is recommended for treatment of patients with symptomatic spinal stenosis associated with low-grade degenerative spondylolisthesis whose symptoms have been recalcitrant to a trial of medical/interventional treatment
Question #14: Does surgical decompression alone improve surgical outcomes in the treatment of degenerative lumbar spondylolisthesis compared with medical/ interventional treatment alone or the natural history of the disease? • Direct surgical decompression is recommended for treatment of patients with symptomatic spinal stenosis associated with low-grade degenerative lumbar spondylolisthesis whose symptoms have been recalcitrant to a trial of medical/interventional treatment. • Indirect surgical decompression is recommended for treatment of patients with symptomatic spinal stenosis associated with low-grade degenerative lumbar spondylolisthesis whose symptoms have been recalcitrant to a trial of medical/interventional treatment.
Question #15: Does the addition of lumbar fusion, with or without instrumentation, to surgical decompression improve surgical outcomes in the treatment of degenerative lumbar spondylolisthesis compared with treatment by decompression alone? • Surgical decompression with fusion is recommended for the treatment of patients with symptomatic spinal stenosis and degenerative lumbar spondylolisthesis to improve clinical outcomes compared with decompression alone
Question #16: Does the addition of instrumentation to decompression and fusion for degenerative lumbar spondylolisthesis improve surgical outcomes compared with decompression and fusion alone? • The addition of instrumentation is recommended to improve fusion rates in patients with symptomatic spinal stenosis and degenerative lumbar spondylolisthesis. • The addition of instrumentation is not recommended to improve clinical outcomes for the treatment of patients with symptomatic spinal stenosis and degenerative lumbar spondylolisthesis.
Question #17: How do outcomes of decompression with posterolateral fusion compare with those for 360 fusion in the treatment of degenerative lumbar spondylolisthesis? • Because of the paucity of literature addressing this question, the work group was unable to generate a recommendation to answer this question.
Posterolateral fusion
360 fusion / interbody fusion
Question #18: What is the role of reduction (deliberate attempt to reduce via surgical technique) with fusion in the treatment of degenerative lumbar spondylolisthesis? • Reduction with fusion and internal fixation of patients with low-grade degenerative lumbar spondylolisthesis is not recommended to improve clinical outcomes.
Question #19: What is the long-term result (4+ years) of surgical management of degenerative lumbar spondylolisthesis? • Decompression and fusion are recommended as a means to provide satisfactory long-term results for the treatment of patients with symptomatic spinal stenosis and degenerative lumbar spondylolisthesis.
Key Points 1 • Spondylosis is a defect in the pars interarticularis. Unilateral defects almost never progress to olisthesis. • Spondylolisthesis is divided into six types. The most common is isthmic (L 5 -S 1 level), followed by degenerative (L 4 -L 5 level).
Key points 2 • Isthmic spondylolisthesis can present in childhood or in adults. • Pediatric – Low-grade disease (<50% slip) typically responds to onoperative treatment. – High-grade disease should be treated with prophylactic fusion. This often requires in situ bilateral posterolateral fusion from L 4 S 1. • Adult – Associated with an increased pelvic incidence. – Operative treatment includes in situ L 4 or L 5 -S 1 posterolateral fusion.
Key points 3 • Degenerative spondylolisthesis is four to five times more common in women and more common in African Americans and diabetics. • It presents as symptoms of central and lateral recess spinal stenosis. • Operative treatment for degenerative spondylolisthesis involves decompression of the nerve roots and stabilization by posterolateral fusion. • Outcomes from the SPORT trial (4 -year follow-up): • Significant improvement in pain and function for operative compared with nonoperative groups
Reference • Mark Miller. Review of Orthopaedics 6 th Edition. • Adam L. Wollowick, Vishal Sarwahi. Spondylolisthesis: Diagnosis, Non-Surgical Management, and Surgical Techniques. • Marchetti PC, Bartolozzi P (1997) Classification of spondylolisthesis as a guideline for treatment. In: Bridwell KH, De. Wald RL, Hammerberg KW, et al. , (eds) The textbook of spinal surgery, 2 edn. Lippincott-Raven, Philadelphia pp 1211– 1254 • Watters WC 3 rd, Bono CM, Gilbert TJ, et al. North American Spine Society. An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spondylolisthesis. Spine J. 2009 Jul; 9(7): 609 -14.