Role of Amylin and Glucagon in Postprandial Glycemic



 • Amylin is a ß-cell hormone co-secreted with insulin. • In")




 Sex (M/F) Ht (m) Controls 15 ± 0. 5 6/5")
 200 50 100 25")


- Slides: 19
Role of Amylin and Glucagon in Postprandial Glycemic Excursions in Pediatric Type 1 Diabetes. Rubina Heptulla MD, Luisa M. Rodriguez MD and Morey W. Haymond MD. Baylor College of Medicine Houston, TX.
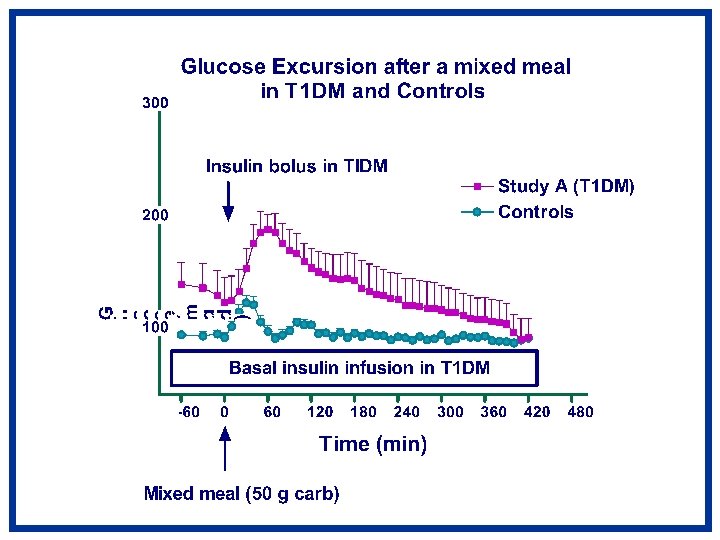
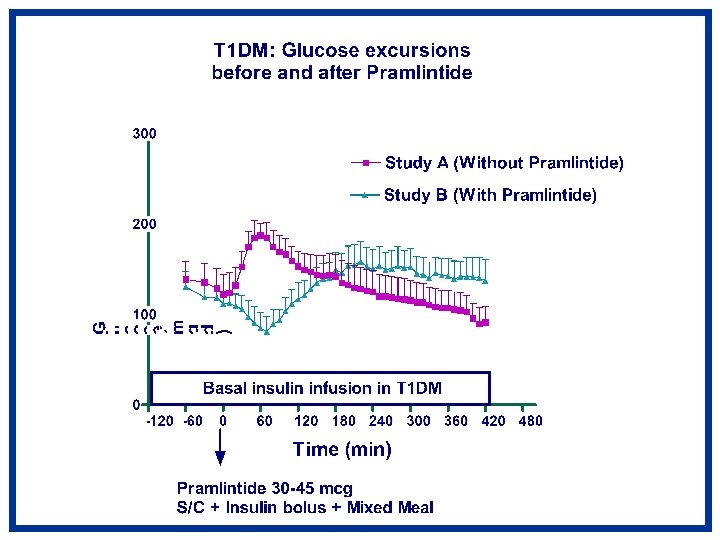
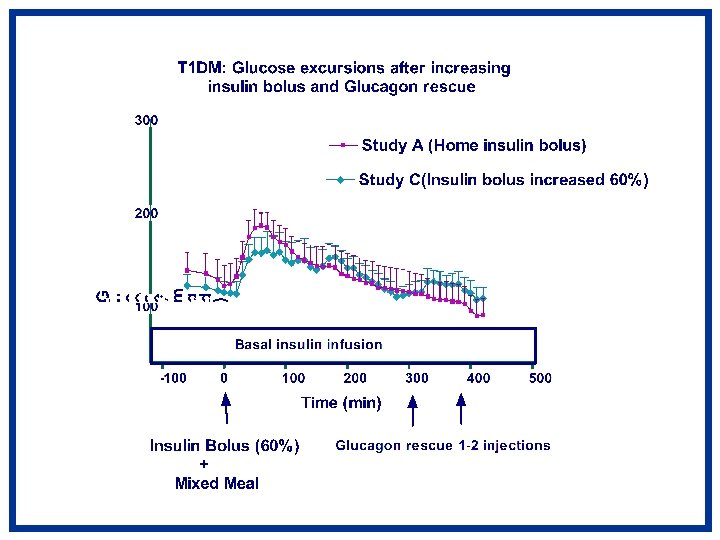
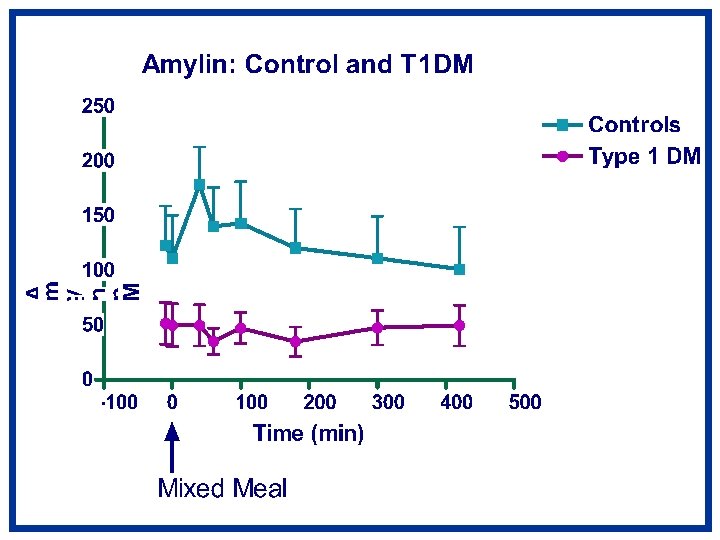
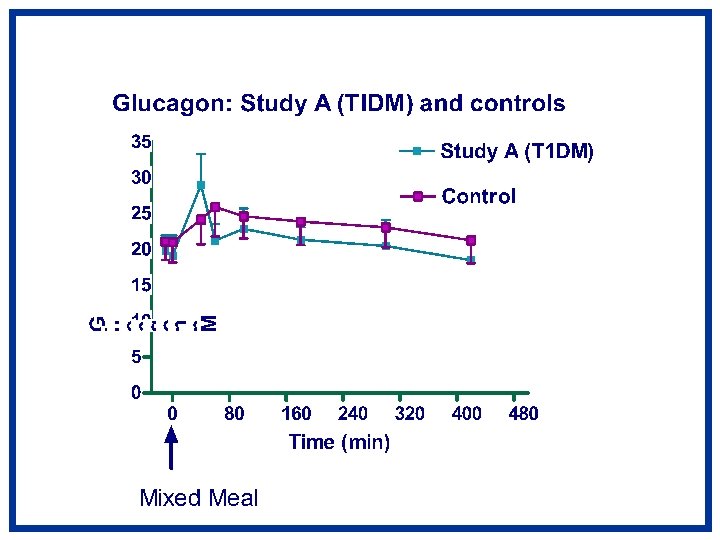
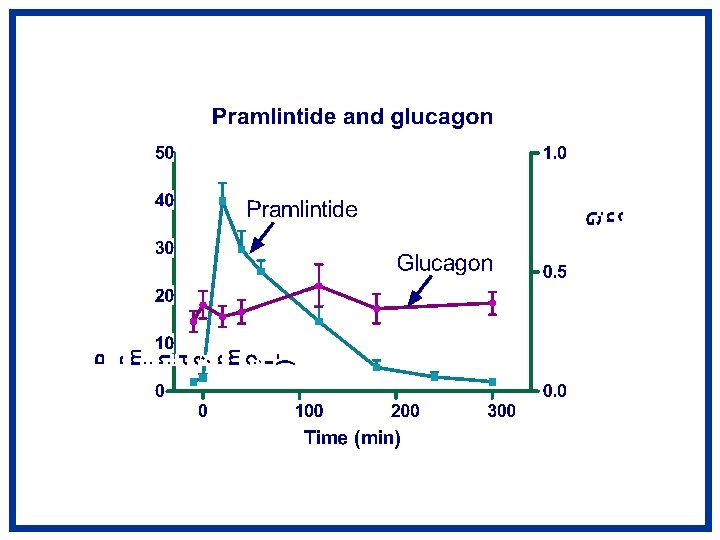
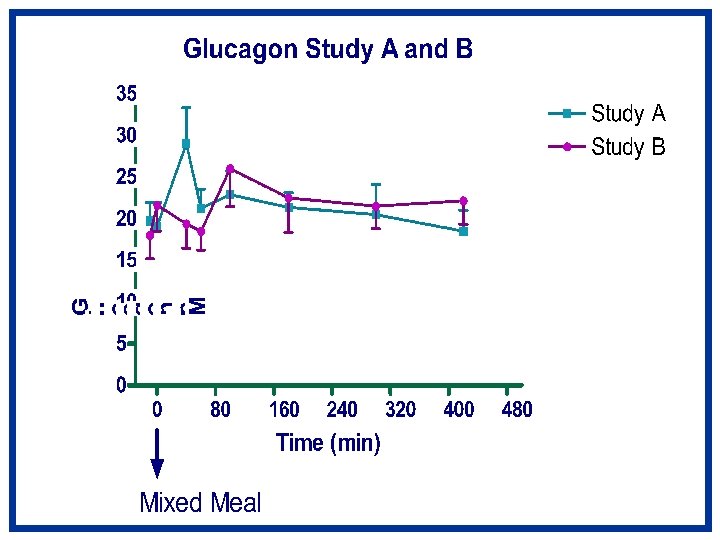
Abstract PP hyperglycemia and pre-prandial hypoglycemia impede optimal glycemic control in Type 1 diabetes (T 1 D). Amylin is secreted by Β cells. T 1 D subjects are amylin and insulin deficient. Amylin in PP period suppresses glucagon and delays gastric emptying. Thus it may play a role in improving PP blood glucose (BG). Pramlintide is a synthetic analog of amylin. We hypothesized that 1. Pramlintide replacement would normalize immediate PP BG in T 1 D and 2. Increased insulin dosage would correct immediate PP hyperglycemia however rescue glucagon injections would be required to prevent hypoglycemia. Methods: 7 adolescents with T 1 D (5 M/2 F, Hb. A 1 C < 8%) on insulin pump were compared to 11 healthy controls. T 1 D subjects underwent 3 studies. Study A: Baseline, subjects were admitted & fasted overnight. Insulin was adjusted to normalize BG. At 7000 (0 min), subjects drank Boost (50 g carb) and received usual insulin bolus. BG, amylin, glucagon and insulin concentrations were measured for 420 min. Study B and C were randomized. Study B: Same as Study A except at 0 min in addition to insulin, S/C injection of pramlintide 30 -45 mcg was given based on insulin sensitivity. Study C: Exactly as study A, except subjects received an increase in insulin bolus by 60% and S/C glucagon rescue (GR) using 5 mcg/kg/dose if BG < 90 mg/dl. Control subjects underwent Study A without insulin. A repeated measures ANOVA was performed. Results: T 1 D had markedly high BG (40% higher) as compared to control (Peak BG: Study A: 194 ± 14, Control 121 ± 6 mg/dl) (p<0. 0001). Study B: Immediate PP BG reduction occurred within 60 min of dose(nadir 84 ± 19 mg/dl), with an escape phenomenon of high BG occurred at 220 min (156 ± 25 mg/dl) (p<0. 0001). Hypoglycemia occurred within 60 min of pramlintide dose in all subjects but one. Increasing insulin dose (study C) decreased immediate PP BG (p<0. 005) and GR prevented hypoglycemia. Conclusions: Our data suggests, S/C pramlintide injection in doses used caused acute PP BG reduction within 60 min. Increasing insulin bolus also lowers BG and hypoglycemia is prevented by rescue doses of GR injections.
Background • T 1 DM is characterized by insulin and amylin deficiency. • Major limiting factors in achieving normal glucose profile in T 1 DM – Postprandial hyperglycemia – preprandial hypoglycemia • Immediate postprandial hyperglycemia – non-physiologic insulin dosing – hyperglucagonemia. • Preprandial hypoglycemia – inadequate glucagon response – iatrogenic affects of insulin.
Pramlintide (Amylin Analog) • Amylin is a ß-cell hormone co-secreted with insulin. • In the immediate postprandial period acts as – glucagon suppressor – delays gastric emptying. • Pramlintide is a synthetic analog of amylin. • Pramlintide replaces amylin agonist activity
Hypotheses in Control Subjects • T 1 DM subjects compared to controls will have – post-prandial hyperglycemia – Pre-prandial hypoglycemia • Normal subjects will have – amylin & glucagon in immediate post-prandial – glucagon & amylin in the late post-prandial
Hypotheses in T 1 DM Subjects • Adjunctive use of pramlintide with insulin in T 1 DM will glucagon & post-prandial hyperglycemia. • Small doses of glucagon post-meal will prevent late post-prandial hypoglycemia
Study Design Controls T 1 DM Study A Study B Study C
Study Design 60% Insulin bolus Study C Insulin Glucagon rescue Insulin bolus+ Pramlintide 30 -45 mcg before meal Glucose rescue Study B Usual Insulin before meal Study A Insulin -300 -240 -180 -120 -60 Blood sugars 90 -140 mg/dl 0 60 120 180 240 300 360 420 Glucose and hormone measurements Subjects admitted overnight Mixed Meal
Study Subjects Age (y) Sex (M/F) Ht (m) Controls 15 ± 0. 5 6/5 1. 68 ± 0. 02 T 1 DM 16 ± 0. 3 6/2 1. 73 ± 0. 02 Wt (kg) BMI (kg/m 2) Hb. A 1 C (%) 61 ± 2 21. 6 ± 0. 6 5. 0 ± 0. 1 64 ± 3 22. 7 ± 0. 9 7. 7 ± 0. 1
Pramlintide PK and Glucose after mixed meal Pramlintide Glucose (mg/dl) 200 50 100 25 0 0 0 40 80 120 160 200 240 280 Time (min) Glucose (mg/dl) Pramlintide p. M 75
Summary • Compared to controls T 1 DM have – Immediate post-prandial hyperglycemia – Late post-prandial hypoglycemia • Adjunctive use of pre-meal pramlintide – postprandial hyperglycemia – 45 mcg dose caused immediate post-prandial hypoglycemia. • A higher insulin dose (60%) pre-meal, minimally improved postprandial hyperglycemia. • Mini dose rescue glucagon prevented late hypoglycemia
Conclusions • Pramlintide appears to have great clinical potential in decreasing post-prandial hyperglycemia • But in some patients, the higher dose can cause immediate post-prandial hypoglycemia • Gastric emptying may play in the acute suppression of glucose absorption • Pramlintide dosing and delivery may need to be modified to prevent hypoglycemia in children with T 1 DM.