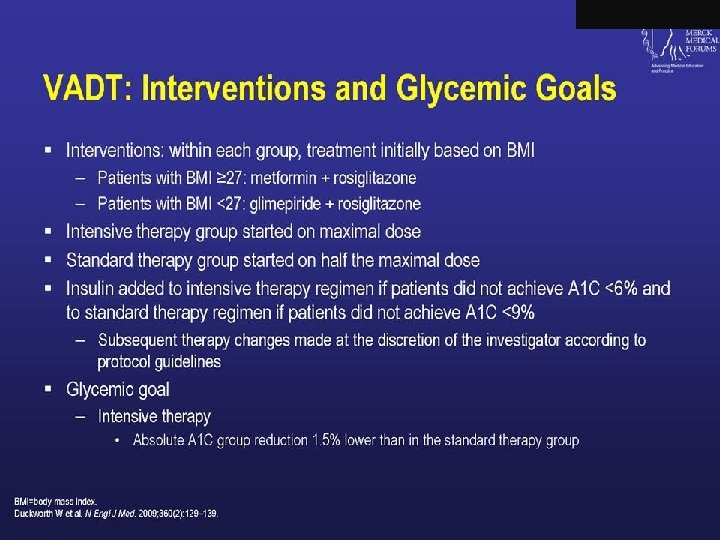
Natural History of Type 2 Diabetes Postprandial Glucose
 250")
Natural History of Type 2 Diabetes Postprandial Glucose 350 300 Glucose (mg/d. L) 250 Fasting Glucose 200 150 100 50 250 Insulin Resistance 200 Relative Function (%) 150 100 50 Prediabetes (IFG, IGT) 0 Insulin Level Clinical Diagnosis Metabolic Syndrome -10 -5 0 Onset Diabetes 5 10 15 Years © 2005. International Diabetes Center, Minneapolis, MN. All rights reserved. 20 25 30

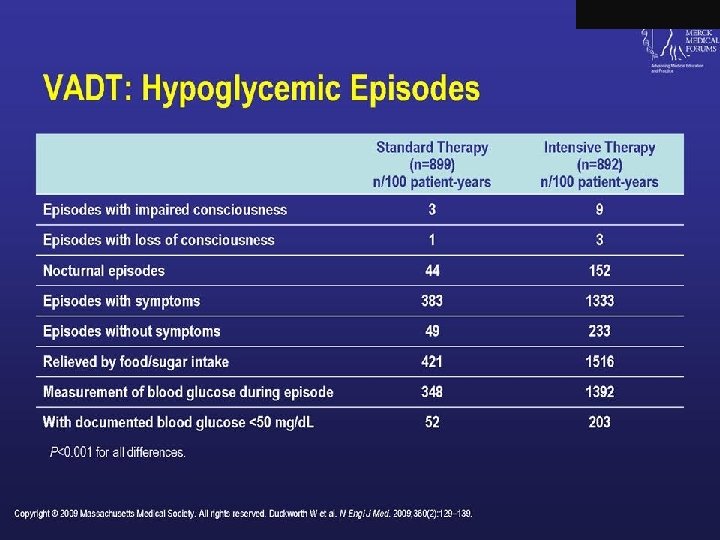
Natural History of Type 2 Diabetes: Disease Progression Genetic Susceptibility Onset of Diabetes Environmental Factors: Nutrition Obesity Physical inactivity IGT Insulin resistance Hyperinsulinemia HDL-C TG Complications Disability Ongoing Hyperglycemia Atherosclerosis Hyperglycemia Hypertension De. Fronzo RA et al. Diabetes Care. 1992; 15: 318 -368. Retinopathy Nephropathy Neuropathy Death Blindness Renal failure CHD Amputation

Pathophysiology of Type 2 Diabetes Increased gastric emptying Carbohydrate Digestive enzymes Glucose Excessive lipolysis (G) I e s o G Gluc I G I (I) G I I G Excess glucose production G I I G G Insulin G Defective -cell secretion G I G Reduced glucose uptake Resistance to the action of insulin
 250")
Natural History of Type 2 Diabetes Postprandial Glucose 350 300 Glucose (mg/d. L) 250 Fasting Glucose 200 150 100 50 250 Insulin Resistance 200 Relative Function (%) 150 100 50 Prediabetes (IFG, IGT) 0 Insulin Level Clinical Diagnosis Metabolic Syndrome -10 -5 0 Onset Diabetes 5 10 15 Years © 2005. International Diabetes Center, Minneapolis, MN. All rights reserved. 20 25 30

Insulin Resistance Is Present Early in the Natural History of Type 2 Diabetes Glucose Uptake (m. L/m 2/min) 400 Nondiabetic/Control Nondiabetic/IGT 300 Type 2 diabetes 200 * 100 0 * *† Normal IGT <144 144 -270 FPG (mg/d. L) *P<. 001 vs normal subjects. †P<. 01 vs IGT and FPG <144 mg/d. L Adapted from Reaven GM et al. Diabetologia. 1989; 32: 52 -55. *† >270

Natural History of Type 2 Diabetes: Disease Progression Genetic Susceptibility Onset of Diabetes Environmental Factors: Nutrition Obesity Physical inactivity IGT Insulin resistance Hyperinsulinemia HDL-C TG Complications Disability Ongoing Hyperglycemia Atherosclerosis Hyperglycemia Hypertension De. Fronzo RA et al. Diabetes Care. 1992; 15: 318 -368. Retinopathy Nephropathy Neuropathy Death Blindness Renal failure CHD Amputation

A 1 C Goals Unmet in Majority of Patients With Diabetes 10. 0 12. 4% have A 1 C >10%1 9. 5 9. 0 A 1 C (%) 8. 5 8. 0 64. 2% of patients with type 2 diabetes have A 1 C 7%2 20. 2% have A 1 C >9% 37. 2% have A 1 C >8% 7. 5 7. 0 6. 5 6. 0 5. 5 1. Data from Saydah SH, et al. JAMA. 2004; 291: 335 -342 2. Calculated from Koro CE, et al. Diabetes Care. 2004; 27: 17 -20 3. Data from ADA. Diabetes Care. 2003; 26(suppl 1): S 33 -S 50 4. Data from ACE. Endocrine Practice. 2002 ADA recommended target (<7%)3 ACE recommended target (<6. 5%)4 Upper limit of normal range (6%)

Patients Remain on Monotherapy >2 Years After First A 1 C >8. 0%* Length of Time Between First Monotherapy A 1 C >8. 0% and Switch/Addition in Therapy* 35. 1 SU Only 26. 5 MET Only 0 6 12 18 Months 24 30 36 SU=sulfonylurea; MET=metformin. *May include uptitration. Based on a prospective, population-based study using retrospective observational data. Brown JB et al. Diabetes Care. 2004; 27: 1535 -1540.

Patients Remain on Monotherapy >2 Years After First A 1 C >8. 0%* Length of Time Between First Monotherapy A 1 C >8. 0% and Switch/Addition in Therapy* 35. 1 SU Only 26. 5 MET Only 0 6 12 18 Months 24 30 36 SU=sulfonylurea; MET=metformin. *May include uptitration. Based on a prospective, population-based study using retrospective observational data. Brown JB et al. Diabetes Care. 2004; 27: 1535 -1540.

Glucose-lowering Potential of Diabetes Therapies* Treatment FPG ¯ A 1 C ¯ Sulfonylureas Metformin/Sulfonylurea a-Glucosidase Inhibitors Repaglinade Thiazolidinediones Exenatide Pramlintide 50 -60 mg/dl 100 -120 mg/dl 15 -30 mg/dl 60 mg/dl 40 -60 mg/dl targets ppd 1 -2% 3 -4% 0. 5 -1% 1. 7% 1 -2% Insulin Unlimited *based on package insert data

Postprandial Glucose Contribution to A 1 c: Closer to A 1 c Goal, the Need to Manage PPG Increases Fasting Plasma Glucose (FPG) Post-Prandial Glucose (PPG) 100 80 Contribution ( %) 30 50 55 60 40 60 70 70 50 20 0 <7. 3 -8. 4 45 40 8. 5 -9. 2 9. 3 -10. 2 A 1 c Range (%) Monnier, et al. Diabetes Care. 2003; 26: 881 -885. 30 >10. 2


Modulation of Insulin and Glucagon Levels: The Enteroinsular Axis Hormonal signals • GLP-1 • GIP Glucagon (GLP-1) Neural signals alpha cells beta cells Pancreas Gut Insulin Nutrient signals Adapted with permission from Creutzfeldt W. Diabetologia. 1979; 16: 75– 85. Copyright © 1979 Springer-Verlag. Drucker DJ. Diabetes Care. 2003; 26: 2929– 2940. Kieffer T et al. Endocr Rev. 1999; 20: 876– 913. Nauck MA et al. Diabetologia. 1993; 36: 741– 744. (GLP-1, GIP)
")
The Incretin Effect in Subjects Without and With Type 2 Diabetes Control Subjects (n=8) 0. 6 Incretin Effect 0. 2 20 0. 1 0 0 60 120 180 Time, min IR Insulin, m. U/L 0. 3 40 60 0. 5 0. 4 0. 3 40 0. 2 20 0. 1 0 0 0 60 120 Time, min Oral glucose load Intravenous (IV) glucose infusion Adapted with permission from Nauck M et al. Diabetologia. 1986; 29: 46– 52. Copyright © 1986 Springer-Verlag. 180 nmol/L 0. 4 0. 6 The incretin effect is diminished in type 2 diabetes. 0. 5 60 0 80 nmol / L IR Insulin, m. U/L 80 Patients With Type 2 Diabetes (n=14)

Insulin Tactics: Starting With Basal Insulin in Type 2 Patients Advantages • 1 injection with no mixing � Can be used with existing oral medications � Slow, safe, and simple titration � Start with low dosage, but remember to titrate � Limited weight gain � Effective improvement in glycemic control

Maximizing Insulin Therapy. Getting Started q. Type 2 adults or adolescents -Add Long acting insulin* to existing oral agents; 10 units starting dose, generally at HS. Titrate upwards 3 units every 5 days until fasting blood glucose at target (<140) q. May be less aggressive for certain populations (elderly) *alternative-premix analog 70/30 or 75/25 or 50/50 with evening meal
- Slides: 49