LUNG CANCER WORLDWIDE The proportion of lung cancer





 of the Chest Routine 938 m. Gy/cm 15. 9 m. Sv")
 •")
 smokers ex-smokers ≥ 30 PA Age 55 -74")











- Slides: 26
LUNG CANCER WORLDWIDE • The proportion of lung cancer patients in developing nations increased from 31% to 49. 9% in the last two decades • 15% of men and 53% of women with lung cancer worldwide are never smokers • Geographic differences: the proportion of lung cancer of never smoking women: • 83% in Asian countries, 15% in US
SCREENING: WHY ? • Goal: cancer mortality reduction • Detect asymptomatic cancers • Asymptomatic cancers = better prognosis (? )
폐암검진의 역사 • 1960 -London Cx. R – No mortality difference • 1970’s – MSKCC, Johns Hopkins, Mayo Cx. R/Sputum – No benefit of adding sputum cytology 1990; s – PLCO- No benefit of Cx. R screening cancer ELCAP – LDCT better than Cx. R at detecting Mayo – LDCT better than Cx. R • 2002 -2004 - NLST – 20%reduyction in mortality LDCT • 2010 – AFB, genomic, proteomic analysis, seruum molecular markers
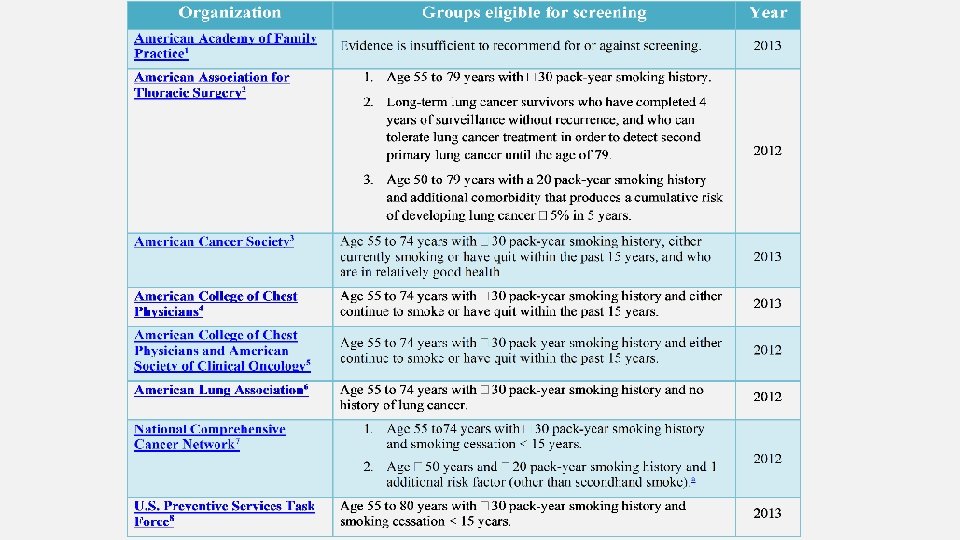
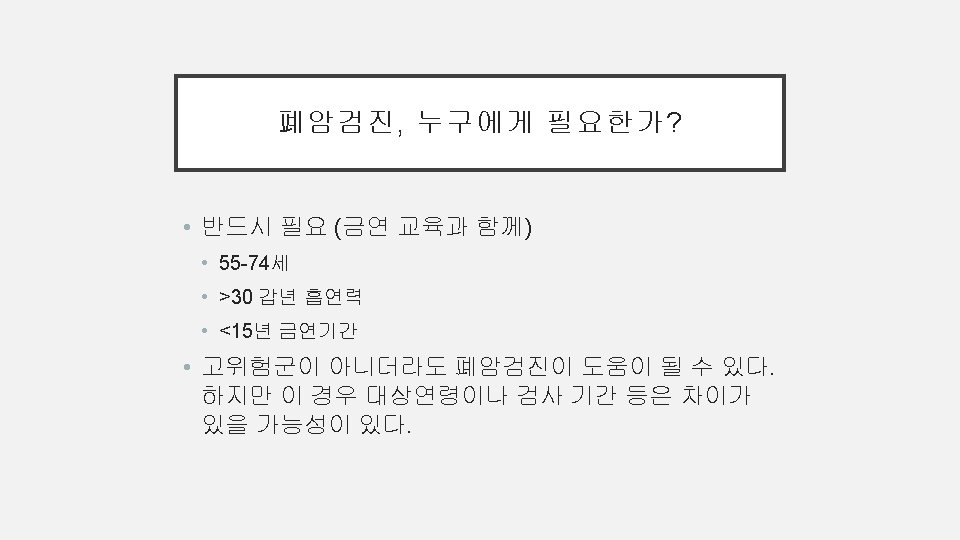
CDC GUIDELINE FOR LUNG CANCER SCREENING Yearly screening with LDCT for people who • Have a history of heavy smoking (>30 PY), and • Smoke now or have quit within the past 15 years, and • Are between 55 and 80 years old
LUNG CANCER SCREENING TOOLS • Sputum Cytology • Chest X-ray Bach, ACCP guidelines, Chest 2007; 132: 69 S-77 S
Computed Tomography (CT) of the Chest Routine 938 m. Gy/cm 15. 9 m. Sv Low-dose 88 m. Gy/cm 1. 5 m. Sv Smith-Bindman, N Engl J Med 2010; 10. 1056
Screening with Low-dose CT It works ? • 31, 567 subjects (1993 -2005) • 481 lung cancers detected • 85% stage I (n=412) ELCAP, NEJM 2006; 355: 1763 -71
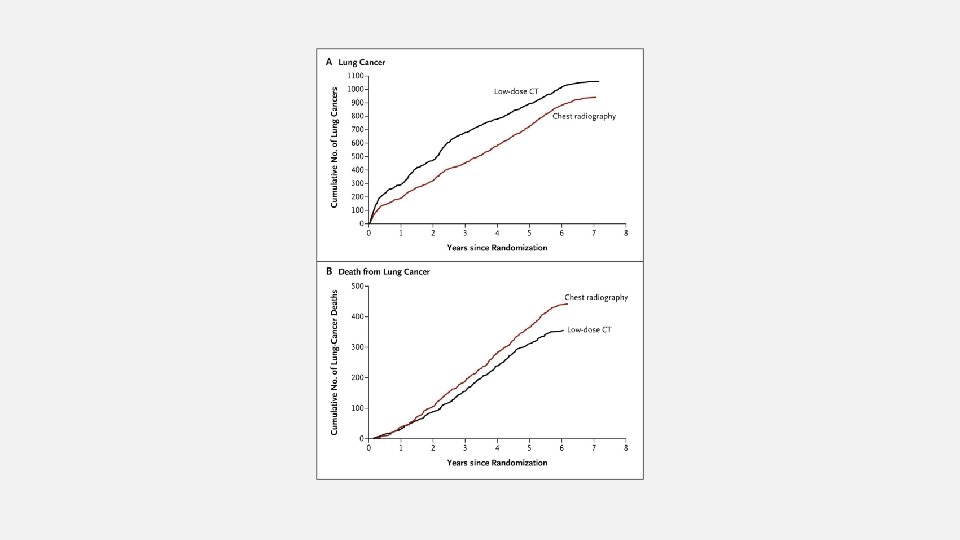
National Lung Cancer Screening Trial (NLST) smokers ex-smokers ≥ 30 PA Age 55 -74 R A N D O M I S A T I O N LDCT Chest PA 0 1 2 Years NLST, NEJM 2011; 365(5): 395 -409
55 to 74 yrs, > 30 P-Y, active or stop<15 yrs n Lung cancers Lung cancer deaths 18. 146 (68. 5%) 1. 060 346 (1. 3%) 5. 043 (19. 2%) 941 « Positive » (diam>=4 mm) Low-dose CT 26. 455 Chest X-ray 26. 232 425 (1. 6%) Risk reduction 20, 0% NNS to prevent 1 lung cancer death = 320… NLST, NEJM 2011; 365(5): 395 -409
NLST: Highly selected population • Probably healthier vs. base population • < 65 years • 73% vs 65% in the base population • Less current smokers • 48% vs 57% • Better educated • 6% with less than a high school education vs 21% NLST, JNCI 2010
European Screening Trials Overview NELSON DLCST ITALUNG LUSI DANTE MILD 4 5 5 10 or 5 Enrollement 15, 464 4, 104 3, 206 3, 551 2, 472 3, 581 Completed Y Y Y N Baseline detection 0. 9% 0. 8% 1. 5% 1. 0% 2. 2% 0. 8% Incidence 0. 5% 0. 6% 0. 4% - 0. 5% Nr rounds de Koning, ECCO-ESMO meeting, Sept. 2011
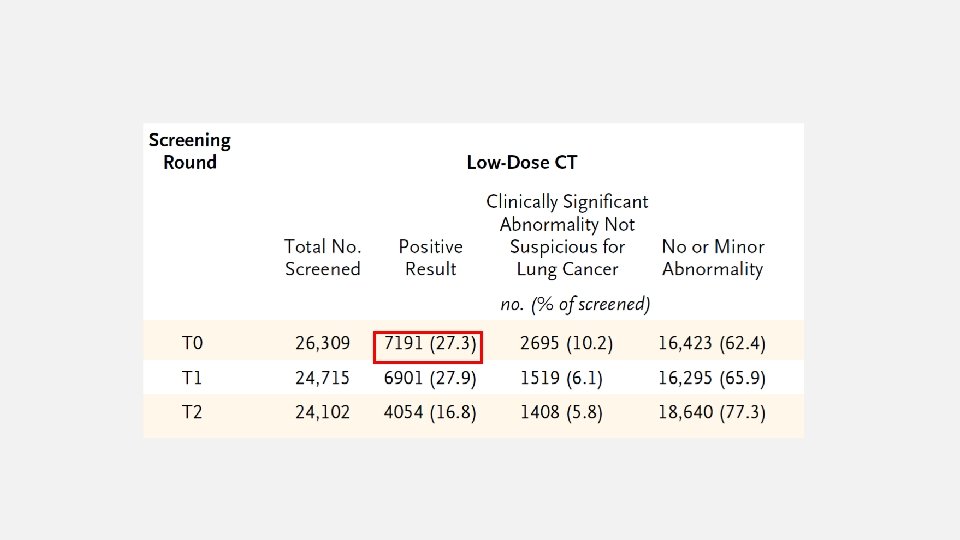
HOW MANY SCREEN ROUNDS? • Lung cancer was diagnosed frequently after the third low-dose CT screening • This observation suggests that continuing to screen high-risk individuals annually will provide a net benefit.
LINEAR NON-THRESHOLD MODEL • CT with an effective dose of 10 m. Sv • Increased risk of fatal cancer of 1 in 2000 • Natural incidence of fatal cancer 400 in 2000 (in the US population)
RADIATION DOSE IN ADULTS Procedure Abdomen and pelvic CT, preand post contrast Brain CT Chest CT Low dose CT Chest PA Coronary CT DEXA PET/CT Mammography Approximate effective dose Comparable natural background radiation 10 m. Sv 20 m. Sv 3 years 7 years 2 m. Sv 7 m. Sv 1. 5 m. Sv 0. 1 m. Sv 8 months 2 years 6 months 10 days 12 m. Sv 0. 001 m. Sv 25 m. Sv 0. 4 m. Sv 4 years 3 hours 8 years 7 weeks
NON-SMOKING LUNG CANCER PATIENTS • Adenocarcinoma, especially bronchioloalveolar carcinoma • Asian ethnicity • Female • Better response to Epithelium Growth Factor Receptor (EGFR) Tyrosine Kinase (TK) inhibitors, such as erlotinib and gefitinib
ETIOLOGIC AND MOLECULAR FEATURES • Several etiologic factors have been proposed: • Occupational and environmental factors: exposure to radon, asbestos, heavy metals • Cooking fumes • Environmental tobacco smoke • Human papilloma virus (HPV) infection • Inherited genetic susceptibility • Molecular features • EGFR mutations, p 53 mutations, K-ras mutations
EXPOSURE TO COOKING FUMES • A meta-analysis reported an increased risk of lung cancer in China • Exposure to domestic coal for heating and cooking • Indoor exposure to coal dust and chronic exposure to cooking oil vapor, though publication bias might affect these two factors • More cooking dish-years, higher the OR of lung cancer • Different frying methods: deep-frying have the highest risk
SUBSOLID NODULES
THANK YOU