General Approach in Investigation of Haemostasis Platelets aggregation








 q The lumi-aggregometer may be used to simultaneously measure")
 q The Platelet-rich plasma, which is turbid in")
 baseline, 2) agonist addition")

 Biphasic curve: 1 o")






- Slides: 20
General Approach in Investigation of Haemostasis Platelets aggregation
Studying Platelets Disorders �Numbers � CBC � � PLT count PLT morphology �Function � Bleeding Time (BT) � Platelet Aggregation � � Whole blood aggregation Platelet-rich plasma aggregation
Platelets contribute to Hemostasis in two main ways: q Primary haemostatic plug : q Adhesion q Aggregation q Secretion q Secondary Haemostatic plug: q Procoagulant activities are generated
Platelets granules q Platelets normally contain three major types of granules. q The alpha granules contain fibrinogen, PF 4, factor V, von Willebrand factor. q The dense granules contain ADP or ATP, calcium and serotonin. q lambda granules – similar to lysosomes and contain several hydrolytic enzymes.
Why Platelet aggregation testing q Evaluation of suspected hereditary and acquired disorders of platelet function. q Hereditary platelet function disorders includes q q Rare defects of adhesion (Bernard Soulier syndrome) Rare defects of aggregation (Glanzmann thrombasthenia) More common defects of secretion (alpha or dense granule deficiency, aspirin-like defects, or other primary secretion defects). Acquired platelet function disorders are more common than the hereditary disorders and include druginduced platelet dysfunction (including aspirin, NSAID’s, clopidogrel, antibiotics, various cardiovascular and psychotropic drugs), uremia, and myeloproliferative disorders.
Principle � Using Aggregating agents to induce platelet aggregation or cause platelets to release endogenous ADP, ATP or both. � Platelet aggregation is studied by means of a platelet aggregometer, Used Principle: 1. Photo-optical Method 2. luminescence technology (Platelet Lumiaggregometry) 3. Electrical Impedance Method
AGGREGATING AGENTS
Electrical Impedance Method q These types of analyzers may use citrated whole blood, as the test sample. q As platelets aggregate, the coat an electrode, impeding the electrical current through the analyzer. http: //www. platelet-research. org/3/pfa. htm
Luminescence technology (Platelet Lumi aggregometry) q The lumi-aggregometer may be used to simultaneously measure platelet aggregation and secretion. The instrument records both aggregation and secretion of dense-granule ATP. q The ATP is measured by its reaction with firefly luciferin to give chemiluminescence. The resulting light emission is detected, amplified, and recorded by the instrument. q Performed by using whole blood or PRP. q This modification of aggregation is particularly sensitive to ATP release, and is as+ light sensitive [A] + [B] → [AB◊] → [Products] measure of platelet activation.
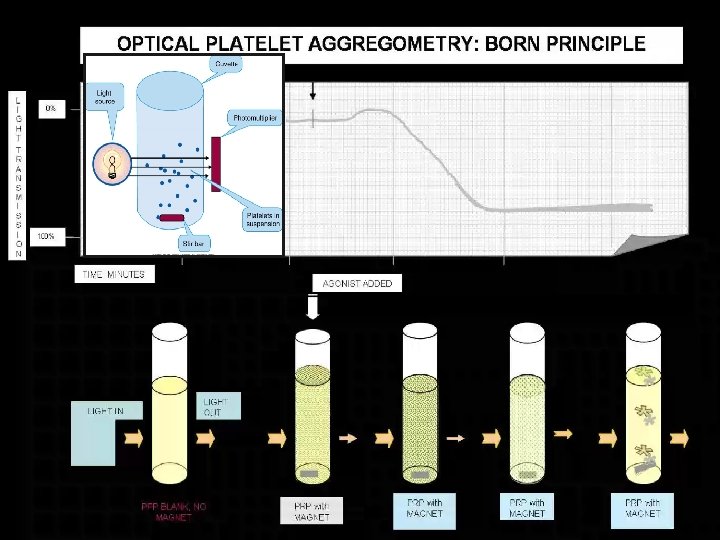
Photo-optical Aggregometer (PLT Aggregometry Using PRP) q The Platelet-rich plasma, which is turbid in appearance, is placed in a cuvettes, warmed to 37°C in the heating block of the instrument, and stirred via a small magnetic bar. q Baseline light transmittance through the platelet-rich plasma is recorded. The addition of an aggregating agent causes the formation of larger platelet aggregates with a corresponding increase in light transmittance, because of a clearing in the platelet-rich plasma. The change in light transmittance is converted to electronic signals and recorded as a tracing by the chart recorder.
Figure 2 – Five possible phases of PLT aggregation: 1) baseline, 2) agonist addition and shape change, 3) primary wave, 4) secretion, and 5) secondary wave.
� Patient Sample – 3. 2% citrated WB � Approximately 20 ml of blood is needed for a full aggregation study. � Test Sample – PRP ( Platelets count fall (200– 600 × 109/L) � Principle – photometry: optical density of PRP warmed to 37° C is determined before and after the addition of various aggregating agents � Issues �Sample quality is critical �Fibrinogen levels are important �Agonists must be prepared fresh daily �Thrombocytopenia makes result interpretation difficult �Complete patient history is essential http: //www. platelet-research. org/3/aggregometry. htm
PRP Aggregometry Agonist & Patterns q ADP (at appropriate concentration) Biphasic curve: 1 o and 2 o waves Note: if ADP is added at too low or too high concentration, it will not get biphasic response q Epinephrine Biphasic curve q Collagen Lag phase followed by 2 o wave only
q Ristocetin A biphasic q Thrombin Biphasic curve. Irreversible aggregation only (does not require cyclooxygenase) q Arachidonic acid 2 o wave only; assesses cyclooxygenase pathway q Serotonin A primary wave of aggregation with a maximum of 10% to 30% transmittance followed by disaggregation.
Interpretation q Platelet aggregation occurs as a two-step process, known as primary and secondary waves of aggregation. q The primary wave of aggregation is observed when platelets adhere to one another in the presence of an external agent (agonist) such as ADP, epinephrine, or ristocetin. q Secondary aggregation is characterized as the aggregation that occurs after the platelets have been stimulated to secrete the substances contained in their organelles. q It should be noted that some agonists will stimulate primary aggregation and some will stimulate
q In addition, different concentrations of the same agonist can produce varying patterns of primary and secondary aggregation. For example, q Low concentrations of ADP induce biphasic aggregation (i. e. , both a primary and a secondary wave of aggregation); q Very low concentrations of ADP (l. 5 ug/ml. final concentration) induce a primary wave followed by disaggregation; q And high concentrations of ADP (10 ug/ml, final concentration) induce a single, broad wave of aggregation“ q Patients with Glanzrnann's thrombasthenia show incomplete aggregation with ADP regardless of the final concentration.
q In patients with severe von Willebrand disease, aggregation to ristocetin is characteristically absent. q Decreased of normal aggregation to ristocetin can be seen in patients with mild von Willebrand disease. q Correction of the abnormal ristocetin aggregation curves can be seen by the addition of normal, platelet-poor plasma to the patient's platelet-rich plasma. q Abnormal ristocetin-induced platelet aggregation may also occur in patients with 1. Bernard-Soulier syndrome, 2. Platelet storage pool defects 3. Idiopathic thrombocytopenia purpura (ITP).
Bernard-Soulier syndrome o Platelet aggregation test o Failure to aggregate in the presence of ristocetin o Aggregation by other agonists (ADP, collagen, epinephrine): normal o Response to low-dose thrombin: may be delayed Platelet storage granule defects o Dense (δ) granule defects ~ storage pool deficiency o α granule defects ~ gray platelet syndrome o Heterogeneous group of disorders o Mild to moderate bleeding diathesis o Abnormalities in platelet aggregation
Precautions Prior To Studying Platelet Aggregation q Aspirin-containing compounds should be excluded for at q q least 10 days prior to testing, as Aspirin interferes with the release reaction. Ingestion of other drugs known to influence platelet function should also be avoided for at least the time required for their elimination from the circulation. These include certain antihistamines, antibiotics, and antidepressants. Lipemia can interfere with the measurement of platelet aggregation, studies should not be carried out shortly after a fatty meal. Many other “normal” dietary constituents, including alcohol, onions, garlic, peppers, and ginger, may also inhibit platelet aggregation. Chilling activates platelets, and so the blood is processed