EVAR Planning Keys to Success Shawn Sarin MD




















 – Radial force, friction")






- Slides: 28
EVAR Planning: Keys to Success Shawn Sarin, MD Vascular and Interventional Radiology The George Washington University Medical Center
Shawn N. Sarin, MD I/we have no real or apparent conflicts of interest to report. Off-Label: Some peripheral intervention devices are off-label.
Planning • Not all patients are candidates for EVAR – Choose the right patients – Patient characteristics and aneurysm anatomy – Only 60% ideal for EVAR based on anatomy • Preprocedural imaging is paramount • Detailed imaging of the aorta – From descending thoracic to common femorals – Nice to know the runoff as well
Pre Procedure Imaging • CTA – 3 D Workstation • MRA • Angiography • IVUS
Develop a Systematic Approach • Visceral and Renal arteries • Proximal Neck Anatomy • Proximal Seal Zone • Distal Neck Anatomy • Distal Seal Zone – CIA/EIA • Access Arteries – CFA/EIA
Visceral and Renal Arteries • Assess patency of Celiac, SMA and IMA • Renal Arteries – Position • In relation to neck • Which is lowest? – Patency – Number
Diameter of Proximal Neck • Measure at the lowest renal and 10 -15 mm below the lowest renal
Measurements • Axial measurements can overestimate due to angulation and tortuosity • Measure diameter perpendicular to central vessel axis
Device Sizing • Oversize neck by 10 -20% – Look at vendor sizing chart • Current devices range from 20 -36 mm and can treat aortic neck diameters from 19 -32 mm • Remember: – Undersized graft may have no seal – Oversized graft may have pleats/folds
Length of Proximal Neck • Need to create a seal between the endograft and the aortic wall • 10 -15 mm length
Contour of Proximal Neck • Change in neck size of >10 -15% over its length associated with higher proximal endoleak rate Straight Tapered Reverse Tapered
Quality of Proximal Neck • Calcification • Mural Thrombus • Angulation – Greater than 90 degrees is a risk factor for an endoleak • Extensive calcification increases probability of stent migration
Angulation of Proximal Neck • • Often seen with larger aneurysms Mild <40° Moderate 40 -60° Severe >60°
Tips and Tricks • Assess angulation on preprocedure imaging will help during procedure and optimize endograft placement • Place endograft as close to lowest renal as possible
Craniocaudal Angulation • Most infrarenal necks have 5 -15° cranial angulation
LAO/RAO Angulation • Determine LAO/RAO angulation based on lowest renal
LAO/RAO Angulation • Determine LAO/RAO angulation based on lowest renal
Iliac Arteries • Common/External Iliacs are the location of distal seal • Are they aneurysmal? – rare for EIA to be aneurysmal – consider coiling of IIA when extending to EIA • Distal seal zone: – 10 -15 mm – Oversize 10 -20%
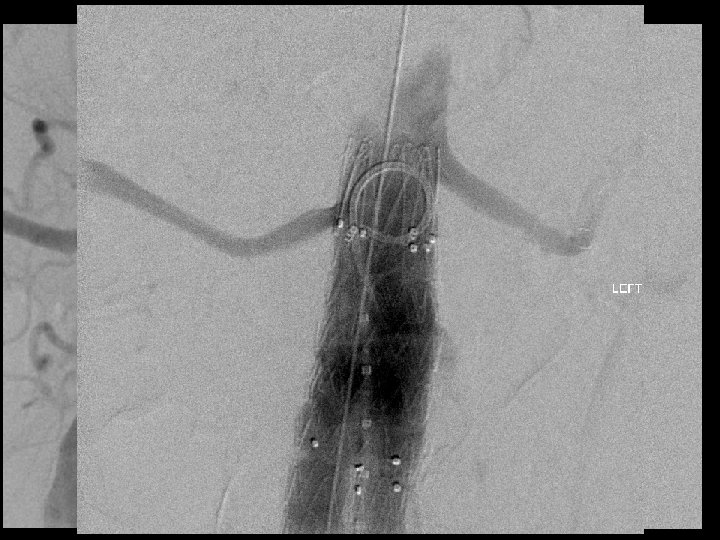
Iliac Arteries
Iliac Arteries • Ideally – Larger than 6 mm – Non calcified – Non tortuous • Newer devices are lower profile and hydrophilic
Graft Selection • Fixation Type – Positive fixation (hooks, barbs) – Radial force, friction – Column support • Sizes • Anatomy • Delivery System – Flexibility – Trackability – OD of delivery system
Graft Selection
Endurant Endologix GORE COOK Proximal neck length 10 mm 15 15 15 neck diameter 19 -32 18 -32 mm 19 -29 mm (inner to inner) 18 -32 mm infrarenal angle <60 <60 access 6. 5 mm/17 18 fr OD 6. 5 mm/17 fr ID/8 12 fr/18 fr/20 fr fr. contralateral 5 mm/6. 8 mm/7. 6 mm 18, 20 and 22 fr OD min access profile (28 mm graft) 20 F OD 19. 2 F OD 23. 1 F OD/18 F OD (LP) 20. 4 F OD
Access Selection • Anatomic factors • Vascular access – Femoral cutdown – Percutaneous
Anesthesia Considerations • General Anesthesia • Regional: – Lumbar – Spinal • Conscious Sediation
Take Home Points • Not all patients are ideal for EVAR as of 2/24/13 • Work in a team • Need a quality pre procedure imaging (CTA) – Helps decide if patient is an EVAR candidate – Device sizing and selection – Aids in intraprocedural planning • Planning will become more important in the future
Thank you! ssarin@gwu. edu