COLOSCOPY UC Early Stage l Hyperemia l Petechial

")
 Stage l Confluating (Continious) l Ulcerations l Pseudopolypo sis")
 Stage l Couble-stone relief l Fissura l Fistula l Solitary")
 Stage l Pseudopolyps l Loss of haustra l Carcinoma")
 Stage l Stenosis l Fistula l Pseudopolyps l Diverticula")










 Oral Aminosalicylates 2) Topical Aminosalicylates 3) Corticosteroids 4) Immunsuppressiva 5) Antibiotics 6)")








![Immunsuppressiva A. B. C. Azathiopyrin (AZT) 6 -Mercaptopurin - Cell replication ] Methotrexat (MTX)](https://slidetodoc.com/presentation_image_h/d3b2e1d41410868e591e161fe565a3b2/image-29.jpg "Immunsuppressiva A. B. C. Azathiopyrin (AZT) 6 -Mercaptopurin - Cell replication ] Methotrexat (MTX)")

 Moderate Corticosteroids (Budesonide) Mild")
 Response 40 -50%")



 in Patients with Fistulizing Crohn’s Disease Complete Response: All")
 Maintenance Studies* Antibody-to-Infliximab (ATI) Status % of Pts with ATI")












- Slides: 49
COLOSCOPY UC Early Stage l Hyperemia l Petechial Bleeding l Fragiability
COLOSCOPY CD Early Stage l Aphtoid l Mucosal Lesions (Ulcers)
COLOSCOPY UC Floride (Acute) Stage l Confluating (Continious) l Ulcerations l Pseudopolypo sis
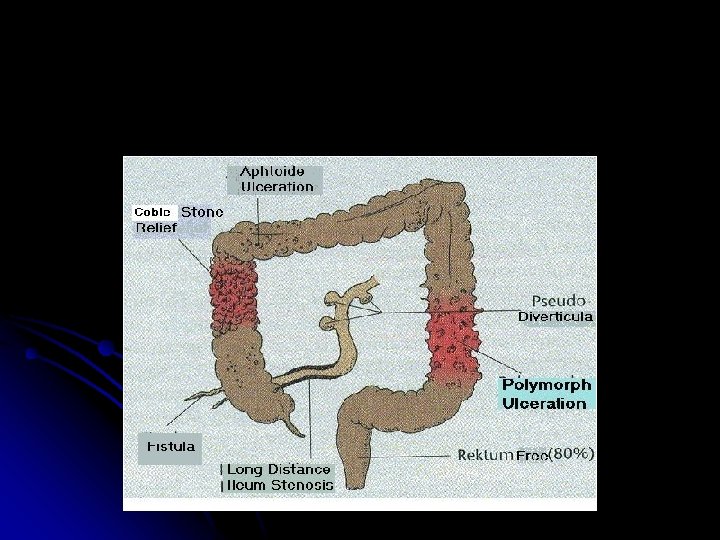
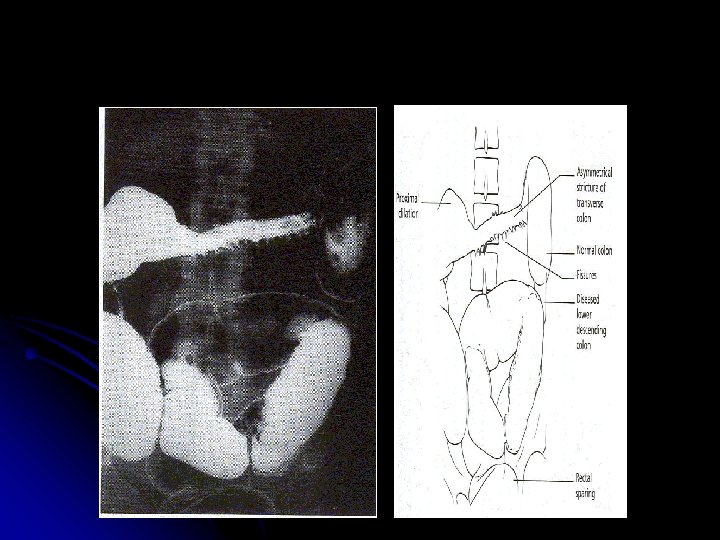
COLOSCOPY CD Floride (Acute) Stage l Couble-stone relief l Fissura l Fistula l Solitary ulcers
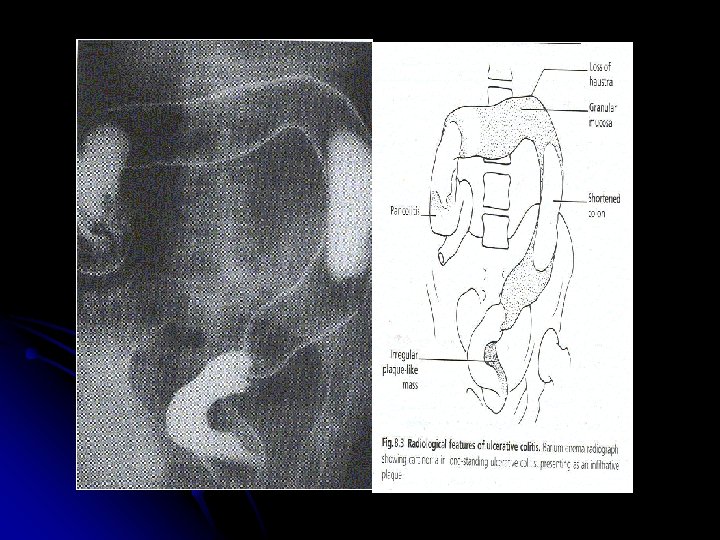
COLOSCOPY UC Late (chronic) Stage l Pseudopolyps l Loss of haustra l Carcinoma
COLOSCOPY CD Late (chronic) Stage l Stenosis l Fistula l Pseudopolyps l Diverticula
Radiology / CD l Couble stone l Aphtoid ulcers l Pseudodiverticula l Fistula l Polymorph ulcers
Activity Index Basedon - Clinical Activity - Endoscopical Activity - Histological Activity - Laboratory Activity
Activity Index /CD
Activity Index /UC
Differential Diagnosis
Prognosis / UC l 80% chronic intermittant l 15% chronic continious l 10% acute fulminant The longer the chronicity The worse is the prognosis.
Prognosis / CD “ No absolute cure” l MILD 30% Remission İn 1 year 70% Remission In 2 years 50% Remission • 70% - Surgical Intervention POSTOP Refall 1 year 70% 2 years 50% l MODERATE
Summary -Prognosis / UC Ø High Rezidive – Quotient Ø Good if isolated Proctosigmoiditis Ø Pancolitis HIGH – Risk often OP.
Summary - Prognosis / CD Ø High – Rezidive Quotient Ø Complications OP
Goals of Therapy for IBD l Inducing remission l Maintaining remission l Restoring and maintaining nutrition l Maintaining patient’s quality of life l Surgical intervention (selection of optimal time for surgery)
Pharma-Information 1) Oral Aminosalicylates 2) Topical Aminosalicylates 3) Corticosteroids 4) Immunsuppressiva 5) Antibiotics 6) Biologic agents (anti TNF-alfa)
Oral Aminosalicylates A. l SULFASALACIN COLON - Sulfapyridine – Carrier + - 5 -ASA – Antiinflammatuar 5 -ASA : 3 -6 g/d INHIBITION - cyclooxygenase - lipooxygenase O 2 -Radical - neutrophil Clearance NK-ABsynthesis depression
Sulfasalacin Sulfapyridine - AZO-BINDING- Azoreductase COECUM 5 -ASA
Oral Aminosalicylates B. MESALAMIN Ileum 5 -ASA Colon 2 g/d Eudragit Capsel
Topical Aminosalicylates l 5 -ASA – FOAM SUPPOSITOIRES
CORTICOSTEROIDS ORAL IV use TOPICAL Prednisone 60/50/40. . . 10 mg Or Less side effected new forms Budesonid 9 mg/d (Endocort / Budenofalk)
CORTICOSTEROIDS l Inhibition of : Proinflammatory Cytokines l Supportion of protective CK. (IL-4, IL 10) l Inhibition of Inflammation Mediators (PAF)
Corticosteroids in CD: Induction of Remission p not calculated 100 92% † 82%* Corticosteroids Placebo % Patients 80 60 60%* 40 30% 38% 20 0 NCCDS ECCDS 17 weeks 18 weeks GETAID 7 weeks Clinical Remission *Randomized controlled trial †Multicenter prospective trial Malchow H et al. Gastroenterology. 1984; 86: 249. Modigliani R et al. Gastroenterology. 1990; 98: 811. Summers RW et al. Gastroenterology. 1979; 77: 847.
Remission Rates in Acute Crohn’s Studies with Budesonide CIR Remission rates at 8 weeks (%) 70 60 50 40 30 20 10 0 Bud CIR 9 mg QD Bud CIR 4. 5 mg BID Placebo 2 g BID Greenberg 1994; Rutgeerts 1994; Thomsen 1998 Pentasa® 40 mg Prednisolone
Immunsuppressiva A. B. C. Azathiopyrin (AZT) 6 -Mercaptopurin - Cell replication ] Methotrexat (MTX) - Antimetabolite - Inhibition of Dihydrofolacid reductase + Lymphocytic Proliferation Cyclosporin - Immunmodulater - T-Cell depression
Antibiotics • Metronidazol
Therapeutic Pyramid for Active Crohn’s Disease Surgery Severe Immunomodulators (Prednisone) Moderate Corticosteroids (Budesonide) Mild Aminosalicylates/Antibiotics Infliximab ?
Outcomes for Mild-Moderate Disease Aminosalicylate Response 40 -50% Antibiotic (Colonic Disease) Response 40 -50% Budesonide (Ileum-Right Colon) Response 50 -65% Placebo Response 30 -40%
Biologic agents • İnfliximap • adaluminap
Infliximab: Mechanism of Action
Healing of Colonic Ulceration with Infliximab Pretreatment Van Dullemen HM et al. Gastroenterology 1995; 109: 129 -135 4 weeks post-treatment
Present, et al. REMICADE® (infliximab) in Patients with Fistulizing Crohn’s Disease Complete Response: All Fistulas Closed P=0. 04 P=0. 001 * *Placebo=Conventional Therapy Present D, et al. N Engl J Med. 1999; 340: 1398 -1405.
Incidence of Antibodies-to-Infliximab (ATI) Maintenance Studies* Antibody-to-Infliximab (ATI) Status % of Pts with ATI n = 514 Week 72 ACCENT I CD * pts with evaluable samples % of Patients Inconclusive† n = 258 Week 54 ACCENT II CD % of Pts without ATI n = 295 Week 102 ATTRACT RA Maintenance Studies † pts with long-lasting serum concentrations of infliximab and never ATI (+) ASPIRE: Integrated Safety Summary, Sep. 18, 2003 n = 629 Week 54 ASPIRE RA
Infliximab indicated Exclude enteric pathogen l Exclude abscess, stricture l Exclude latent/active TB l (Start 6 -MP/AZA or MTX) Response Infliximab 5 mg/kg wks 0, 2, 6 l Consider steroid pre-treatment l Consider acetaminophen, diphenhydramine pre-treatment Observe up to 8 wks Recurrent sx ≤ 4 wks Recurrent sx > 4 - < 8 wks Recurrent sx ≥ 8 wks Inadequate response Maintain infliximab 5 mg/kg q 4 -8 wks Infliximab 10 mg/kg Inadequate response Surgery or investigational Rx Inadequate response Escalate dose or shorten interval Loss of response Maintain infliximab 5 mg/kg q 8 wks
Medical Management / CD Long-term Therapy : A – IMMUNSUPPRESSIVA A 2 T : 25/50 MG Tbl. + - CS for Relapsing Falls B – SURGERY Remissions – maintenance - 5. ASA : 2 g/d 2 years
Methotrexate
Historical Overview l 1948 – first “designer drug” specific antagonist of folic acid l 1950’s – serendipitous discovery of activity in psoriasis l 1960’s – widely used for psoriasis – hepatotoxic l 1966 – Enderlin reported use in RA l 1985 – Wienblatt defines pharmacokinetics in RA l 1980 -2000 for RA – treatment of choice
MTX Results: Remission 50 % Response P =0. 025 25 0 19. 1% Placebo Feagan. N Eng J Med. 1995; 332(5): 292 -7 39. 4% MTX
Methotrexate in IBD: Toxicity l Major l Minor l Hepatic l Gastrointestinal l Myelosuppressive l Alopecia-inductive l Pulmonary l Allergic l Fertility-related l Neurologic l Teratogenic l Enteritic/colitic Egan LJ, Sandborn WJ. Mayo Clin Proc 1996; 71: 69 -80
CD: Moderate to Severe Moderate CD Observe Success Taper Adequate response Failure PO Steroids Severe CD Adequate response Inadequate response 6 -MP/AZA Adequate response Maintain 6 -MP/AZA or MTX Maintain infliximab + 6 -MP/AZA or MTX Adequate response IV Steroids Inadequate response/intolerant Consider change to MTX Inadequate response/intolerant Add infliximab Inadequate response/intolerant Surgery or investigational therapy Inadequate response l. Consider infliximab + 6 -MP/AZA or MTX l. Consider surgery
Medical Management / UC l Refractory States or Chronic active Forms l Immunsuppressiva A 2 T : +? Cs OP Proctocolectomy (= Definitive Cure)
Ulcerative Colitis l Remissions l 5 -ASA – Maintenance 2 gr/d
OP – Indications / CD Bleeding l Ileus l Stenosis l Fistula l Carcinom l Perforation l Abcess l
OP – Indications / UC l Toxic Megacolon l Perforation l Severe Bleeding