Anesthetic Considerations for Evoked Potential Monitoring in Neurosurgery


 than EEG wave (50 -100 μV) n Extracted")




 n Somatosensory-evoked potentials (SSEP) n Brainstem auditory-evoked potentials")




, short latency (<10 msec), high frequency,")
 waves: brainstem function n Long-latency(>10 msec) waves: cortical function -early cortical")



 Unconscious processing of auditory information and implicit memory of")



 n VEPs are the most sensitive BAEPs")
 Both inhalational and intravenous anesthetic agents result")
 Midazolam causes a ↓ in amplitude without")

 1) Systemic blood pressure m. BP↓: SSEP")
 2) Temperature -Hypothermia: VEP ↑in latency &")
 4) Blood-gas tension severe hypoxia: SSEP ↓in")






- Slides: 39
Anesthetic Considerations for Evoked Potential Monitoring in Neurosurgery School of Medicine Konkuk Universit y Won-kyoung Kwon M. D. Assistant Professor
Evoked potential n A measurement of the electrical potentials produced in response to stimulating the nervous system (evoked) by sensory, electrical, magnetic or cognitive stimulation
Characteristics n Lower amplitude(1 -2 μV) than EEG wave (50 -100 μV) n Extracted from EEG activity by repetitive stimulation and computer-signal averaging techniques
n n n Amplitude: the waves’ peak-to-peak voltage difference Latency: the time from stimulus to the peak of the response Interpeak latency: the interval between the peaks of interest
Negative wave n Positive wave n
Near-field potentials: responses recorded by electrodes near from the neural generator n Far-field potentials: responses recorded by electrodes farther from the neural generator n Short latency < 30 ms n Intermediate latency n Long latency > 75 ms n
SEP and MEP Sensory evoked potentials(SEP) n Somatosensory-evoked potentials (SSEP) n Brainstem auditory-evoked potentials (BAEP) n Visual-evoked potentials(VEP) Motor-evoked potentials(MEP)
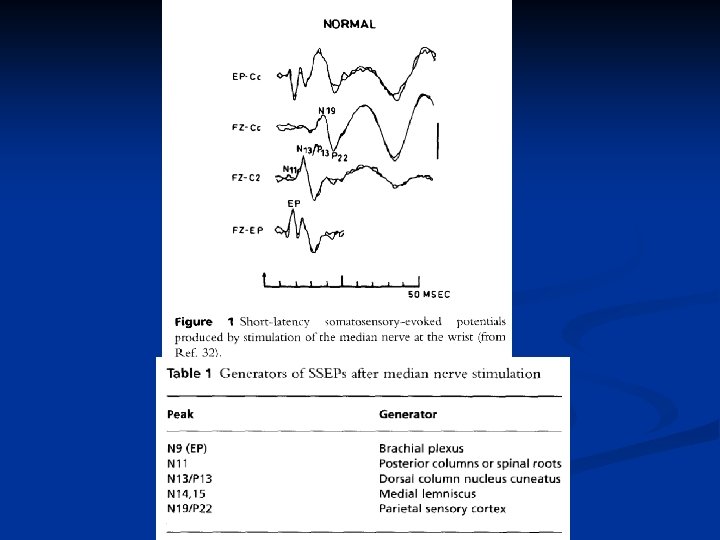
SSEP n The reproducible electrical activity of cortical and subcortical structures timelocked to a peripheral nerve stimulus n The common sites of stimulation: the median n. at the wrist the common peroneal n. at the knee the post. tibial n. at the ankle
A. SSEP after stimulation to the left median nerve B. SSEP after stimulation to the left tibial nerve
Procedures to be monitored n Spinal surgery: esp. scoliosis corrective surgery n Brainstem and cortical surgery n Neuroradiological procedures n Carotid endarterectomy
Warning criteria 30 -50% decrease in the amplitude of potentials n 2. 5 msec increase in the response latency or an increase of 5 -10% of the reponse latency n n False negative and false positive
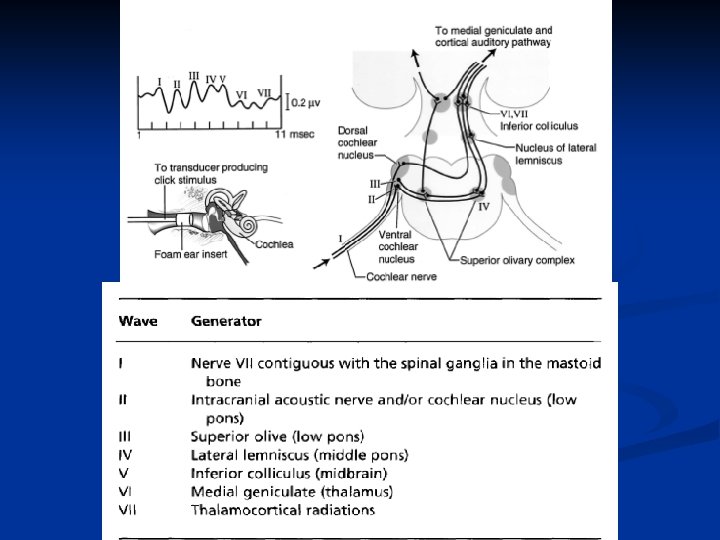
BAEP n Far-field potentials: low amplitude (<0. 1μV), short latency (<10 msec), high frequency, and a wide distribution over the scalp n Low signal-to-noise ratio(SNR)
BAEP Short-latency(<10 msec) waves: brainstem function n Long-latency(>10 msec) waves: cortical function -early cortical or middle latency waves(10100 msec) : generated from the medial geniculate and primary auditory cortex -late cortical waves(>100 msec) : generated from the frontal cortex and associated areas n
Procedures to be monitored Surgery involving or near to the auditory pathway n Posterior fossa surgery n - MVD of CN, resection of acoustic neuroma, exploration for vascular or neoplastic lesions, basilar a. aneurysm, AVM and section of nerve VIII for intractable tinnitus
Causes to result in alterations in BAEP Cerebellar retration n Manipulation of the auditory n. n Tumor dissection and debulking n Patient positioning n Lumbar drainage and dural opening n Hypocarbia, hypotension and ischemia of the cochlea, auditory n. or brainstem n Artifacts n
Warning criteria Prognostic value The usefulness of the BAEP in preserving n Dramatic hearing decreases in amplitude: -Preservation or loss of all components changes in the latency of peak Vof in the BAEP: correlated with presence or range of of 0. 5 -1. 5 msec absence postoperative hearing n Obliteration of wave: -The loss of peaks I and V results in a complete disappearances loss of hearing postoperatively of peak -An amplitude reduction of more than 50% for peaks I and V or the loss of one of the peaks: the best prognosticator of a postoperative hearing deficit V
Middle latency auditory-evoked potential (MLAEP) Unconscious processing of auditory information and implicit memory of intraop. events when early cortical potentials of the MLAEP are preserved during general anesthesia -Pa: implicit memory -Nb: wakefulness and conscious awareness with explicit recall
VEP n Function of the retina, optic chiasm, optic radiation and optic cortex n Recorded after monocular stimulation with recording electrodes over occipital, parietal and central scalp n Surgery for pituitary or cavernous sinus tumors and cerebral aneurysm
Limitations of VEP Difficulty with the delivery of the stimulus n Considerable intrasubject and intersubject variability n
Successful intraoperative monitoring of VEP A new device using high power light emitting diode + TIVA n Induction: propofol 1. 5 -2 mg/kg fentanyl 2μg/kg maintenance: propofol 6 -10 mg/kg/hr additional fentanyl 2μg/kg q 60 min -> from 30% to 84% n Sasaki T et al. Intraoperative monitoring of visual evoked potential: introduction of a clinically useful method. J Neurosurg. 2009 Feb
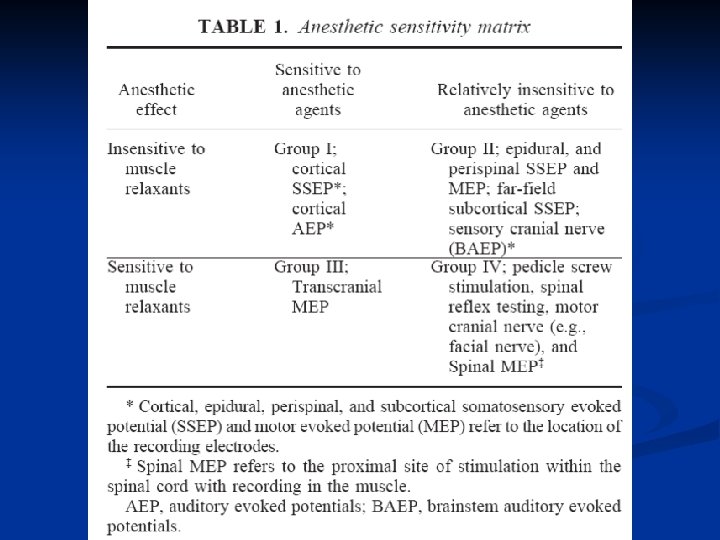
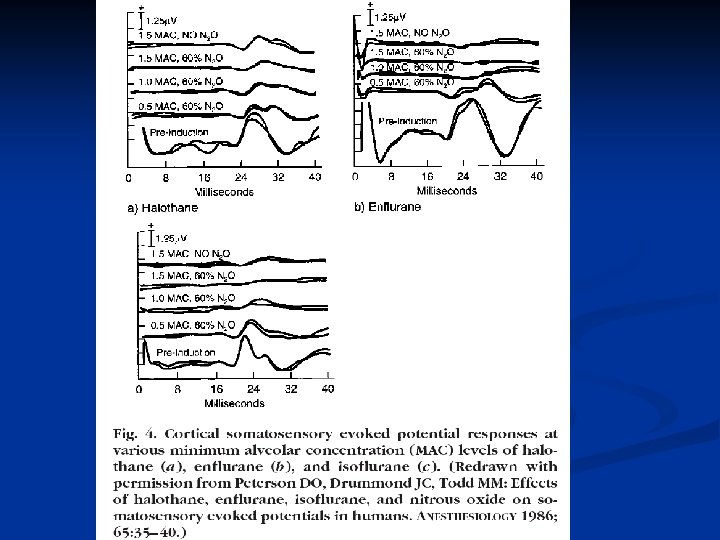
Influence of anesthetic drugs in SEPs (I) n VEPs are the most sensitive BAEPs are the most resistant n Early waves(brainstem) are affected less the are late potentials(cortical) n With inhalational agents, the spinal and subcortical waves are affected less than the cortical potentials
Influence of anesthetic drugs in SEPs (II) Both inhalational and intravenous anesthetic agents result in increase in latency and a reduction in amplitude of the MLAEP n Nitrous oxide produces less effect on the MLAEP n Opioids have little or no effect on the MLAEP n
Influence of anesthetic drugs in SEPs (III) Midazolam causes a ↓ in amplitude without changes in latency of SSEPs n Narcotics cause dose-dependent ↑ in latency and ↓ in amplitude of SSEPs n The effect of volatile agents in SSEPs are dose dependent ↑ in latency and conduction time and ↓ in amplitude n
Drug effects on SEPs
Influence of physiologic factors on SEPs (I) 1) Systemic blood pressure m. BP↓: SSEP ↓ in amplitude & no change in latency BAEP relatively resistant
Influence of physiologic factors on SEPs (II) 2) Temperature -Hypothermia: VEP ↑in latency & ↓in amplitude, loss of waves at 25 -27℃ BAEP ↑in latency and alteration in morphology at 29 ℃ -Hyperthermia: SSEP ↓in amplitude at 42 ℃ BAEP ↓in amplitude & latency
Influence of physiologic factors on SEPs (III) 4) Blood-gas tension severe hypoxia: SSEP ↓in amplitude & ↑in latency hypercapnia>100 mm. Hg: SSEP ↓in amplitude & ↑in latency 5) Isovolemic haemodilution SSEP and VEP ↑in latency
MEP Assess the function of the motor cortex and descending tracts n Types of MEPs n -Transcranial magnetic MEPs (tc. MMEP) -Transcranial electrical MEPs (tc. EMEP) -Direct epidural spinal cord stimulation -Noninvasive spinal cord stimulation: the neurogenic MEPs
Warning criteria More sensitive indicator of potential damage to the spinal cord than SEPs n Magnetic MEP: 50% decrease in the amplitude and a 2. 5 -msec increase in latency n Changes of amplitude are a superior criterion n Neurogenic MEP: 20 -30% decrease in amplitude n
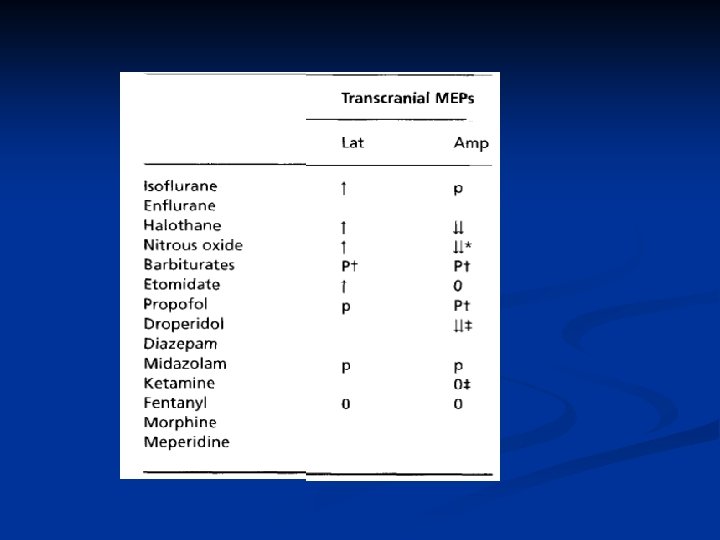
Anesthetic considerations Narcotics have less effect than volatile anesthetics n Neuromuscular blocking drugs may obtund the response completely n
82/F Hx of severe Lt ICA stenosis Lt carotid endarterectom y Trace 7: Rt Trace 8: Lt
47/F Hx of SAH Lt ICA stenting & coiling of aneurysm Trace 7: Rt C 4’-Fz Trace 8: Lt C 3’-Fz
M/42 Hemifacial spasm, MVD