Acne vulgaris Dr Anwar Issa hasan 15112018 Acne






, acne cosmetica or pomade acne")










: recurrent flushing, burning, fixed erythema in central")


 II) Topically • Bland emollient • Anti-acne agents • Topical")

- Slides: 23
Acne vulgaris Dr. Anwar Issa hasan 15/11/2018
Acne vulgaris • Its multifactorial disease of pilosebaceous unit. • Common , occurs in about 85% of individuals 12 -24 years and 15 -35% of adults in their 30 s-40 s (specially women). • Clinically presented with comedones (white & black) , papules, pustules , nodules , cysts and scaring. • Its Subacute , chronic inflammatory disease. • Significant psychological and economic impact.
pathogenesis 1. Genetic: the number, size, activity of sebaceous gland are inherited, also sever nodulocystic acne runs in families. 2. Sebum production : increase sebum production due to hormonal factor(androgens) is contributing factor. 3. Comedo formation: 1 st step in acne formation is follicular hyperkeratosis at upper part of hair follicles. (previously) 4. Inflammatory response: early in acne prone sites show increase in number of CD 4 T lymphocytes & IL 1 increase perifollicularly and cause hyperkeratosis. 5. Propionibacterium acne : grame +ve , anaerobic bacterial flora increase in the number & release lipases witch induce inflammatory response.
Pathogenesis :
Clinical features : v Acne vulgaris: two type of lesions • Non inflammatory : closed or open microcomedones & comedo. • Inflammatory : pink papules, pustules, nodules & cysts. • Sites : face , upper back, chest &upper arms. • Post inflammatory hyperpigmentation & scaring. • Systemic symptoms : in the sever acne variant , acne fulminans , patient has fever , arthralgia &myalgia. • Lab finding : in acne fulminans , increase in ESR, leukocytosis , anemia, microscopic protein urea.
Clinical subtypes 1. Post adolescent acne: age>25, mostly women, flare week prior to the cycle, up to 1/3 of these women have hyperandrogensim, typically papulonodules at lower face , jawline &neck. 2. Acne Excoriee: teenager girls , habitual picking, crusted erosion(linear) & scaring. 3. Acne conglobate : sever , eruptive nodulocystic acne in young male , if there is systemic symptoms called acne fulminans. 4. Neonatal acne : from 2 weeks – 3 months age , cheeks, due to Malassezia spp, resolve spontaneously. 5. Infantile acne: 3 months-2 years, hormonal, classical acne & may scaring.
Clinical subtypes: 6. Contact acne: acne mechanica (chronic friction), acne cosmetica or pomade acne (due to hair oil). 7. Chlorance: result from occupational exposure to the halogenated aromatic hydrocarbons , comedones& cystic papulonodules. 8. Drug induced acne : • Steroid acne: due to systemic CS, follicular , monomorphic , papulopustular, itchy &mostly on back. • EGFR: acne form rash , e. g. cetuximab & erlotinib. 9. Acne associated with syndromes : SAPHO syndrome.
clinical variant of acne
Acne vulgaris
Acne vlugaris
DDX OF ACNE VULGARIS: 1. Comedones: milia , sebaceous hyperplasia, syringomas. 2. Rosacea : papulopustular type. 3. Periorificial dermatitis. 4. Folliculitis ; gram –positive , gram-negative , Demodex &pityrosprum folliculitis. 5. Pseuduofoliculitis barbae. 6. Drug induced acne form eruption. 7. Tinea faciei. 8. Keratosis pilaris. 9. Hidradenitis suppurativa.
Management of acne: Avoidance: oily make up , sunblock's , pomade , harsh soap, psychological stress & skim milk. 1. Topical retinoid ; comedolytic>anti-inflammatory effects, tretinion, adapalene &tazorotene • Initial response 3 -4 weeks , use small amount & treat all acne prone areas. • Causes irritation, so use small amount in alternate night. 1. Topical antimicrobials: benzoyl peroxide and/or antibiotic(clindamycin , erythromycin). 2. Oral antibiotic: 1 st line tetracycline(Doxycycline , minocycline), alt e. g. azithromycin, trimethoprimsulfamethoxazole for 3 -6 months.
Management of acne 3. OCPs: for hormonal acne e. g. Estrostep( ethinyl estradiol 20/30/35 Microgram, norethindrone 1000 Mg) , for 6 months &up to 2 years. 4. Anti androgens: spironolactone 50 -200 mg. 5. Oral isotretinion: systemic retiniods, 0. 5 -1 mg/kg for 4 -6 months. 6. Treatment of acne &scaring : chemical peels, physical treatment e. g. , laser, lights IPL, microneedling radiofrequency.
Treatment of acne Sebum production • • • P. acnes ➢ Hormonal therapy ➢ Antibiotics ➢ Sebum correction ➢ Benzoyl peroxide ➢ isotretinoin ➢ Isotretinoin Follicular hyperkeratinization • Inflammation ➢ Topical retinoids ➢ Antibiotics ➢ Topical tazarotene ➢ Benzoyl peroxide (receptor selective) ➢ Hormonal therapy Isotretinoin ➢
Isotretinion 1. contraindicated in pregnancy : fallow up , pregnancy test each month during treatment, use of two contraceptive methods. 2. Measurement of serum lipid & liver enzymes each month during treatment. 3. It is cause flare up of acne : at the begin of treatment , so we can use prednisolone tab for 2 weeks with isotretinion. 4. This drug cause sever mucositis: so we should advice the patient to regular use of lipstick emollient like Vaseline. 5. Other side effects: musculoskeletal pain. Conjunctivitis & depression.
Rosacea • its chronic, vascular inflammatory disorder, usually limited to the center of face and characterized by recurrent flushing, persistent erythema, telangiectasia, papules and pustules. • Age between 30 -50 years. • Sex: more in females& more in white peoples.
Rosacea Etiology and exacerbating factors • • GIT disturbances. Reaction to the follicular mite, Demodex follilculorum. Climatic (sun). Vasomotor instability. Psychic factors. Role of helicobacter pylori. Rosacea has been reported as a manifestation of HIV infection.
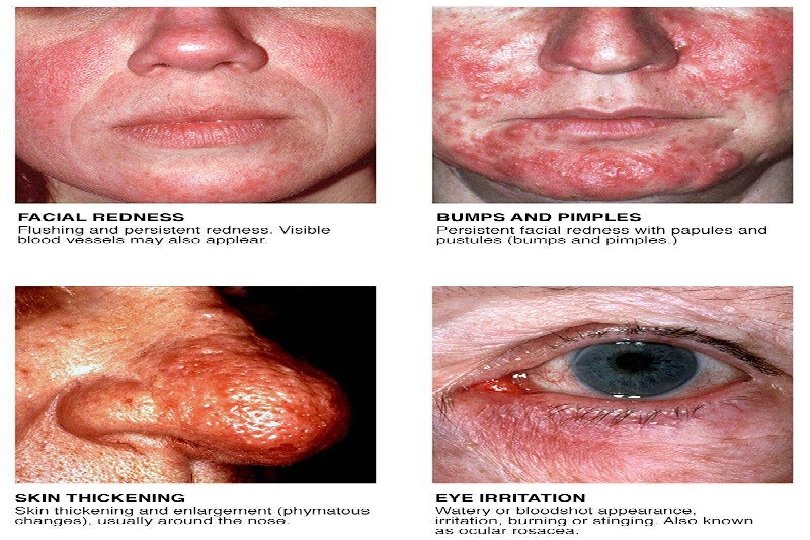
CLINCAL TYPES OF ROSACEA 1. Erthymatotelangiectasic (vascular): recurrent flushing, burning, fixed erythema in central part of face & telangiectasia. 2. Papulopustular rosacea(inflammatory): intermittent pink or red papules and inflammatory pustules. 3. Phymatous rosacea: hypertrophy and irregular(lumpy) thickening of nose(rhinophyma), cheeks, forehead, chin & ears, more in males. 4. Ocular rosacea: burning, foreing body sensation, photophobia& recurrent conjunctivitis& styes.
Rosacea
Rosacea Treatment Avoid extremes of heat & cold, excessive sunlight, spices, hot liquids & alcohols. I) Systemic treatment • Tetracyclines: 250 mg 3 times daily. • Metronidazole (Flagyl®) 200 mg twice daily. • Isotretinion.
Rosacea - Treatment (Cont’d) II) Topically • Bland emollient • Anti-acne agents • Topical metronidazole 0. 75% gel (Metrogel) III)Plastic surgery for rhinophyma&co 2 laser.
Thank you