Psoriasis DR Anwar Issa Hasan M B CH

Psoriasis DR Anwar Issa Hasan M. B. CH. B C. A. B. S-D. V

Psoriasis is a chronic, non-infectious, inflammatory skin disorder, characterized by well-defined salmonpink plaques bearing large adherent silvery centrally attached scales.

• It’s a common chronic skin disease affecting 1_2% of population • It is a life-long disorder with unpredictable remissions & exacerbations. There is no age or sex predilection but common between 15 -40 yrs of age.

PREDILICTION SITES Limbs extensors (elbow, knee_ Sacral region Umblicus Scalp Genital region nails

Causes and pathogenesis The precise cause of psoriasis is still unknown. it appears to be multifactorial. However, there is often a genetic predisposition, and sometimes an obvious environmental trigger.

• A polygenic inheritance is suggested. • Numerous chromosomal loci have been discovered for psoriasis, e. g. PSORS 1 (Psoriasis Susceptibility Loci 1) (major gene) situated within MHC region of chromosome 6 (6 p 21), PSORS 2 17 q, PSORS 3 4 q.

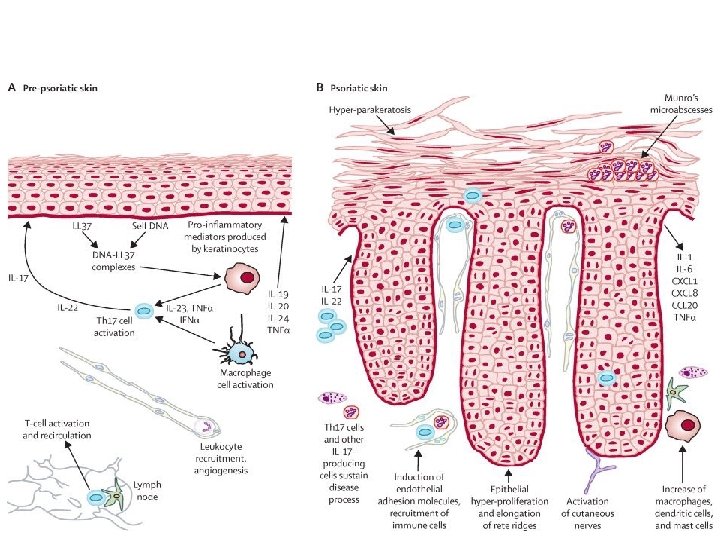
Pathogenesis There are two key abnormalities in a psoriatic plaque: 1. hyperproliferation of keratinocytes 2. inflammatory cell infiltrate in which neutrophils, tumour necrosis factor and probably Th 17 type T lymphocytes predominate.

Provocative factors • Trauma: lesions can appear in skin damaged by scratches or surgical wounds – (the Köbner phenomenon) • Infections, Tonsillitis caused by â-haemolytic streptococci often triggers guttate psoriasis. • Weather: psoriatic patients get worse in winter • hormonal factors: Psoriasis frequently improves in pregnancy only to relapse postpartum. • Drugs, Antimalarials, beta-blockers, IFN-á and lithium may worsen psoriasis. • Emotional stress: tended to aggravate psoriasis in 40% of cases. • Cigarette smoking and alcohol: Psoriasis is more common in smokers and ex-smokers but cause and effect relationships are uncertain.

• The Koebner phenomenon, i. e. the elicitation of psoriatic lesions by injury to the skin, is observed in approximately 25% of patients with psoriasis • psoriasis.

Auspitzs sign: the appearance of punctate bleeding spots when psoriasis scales are scraped off

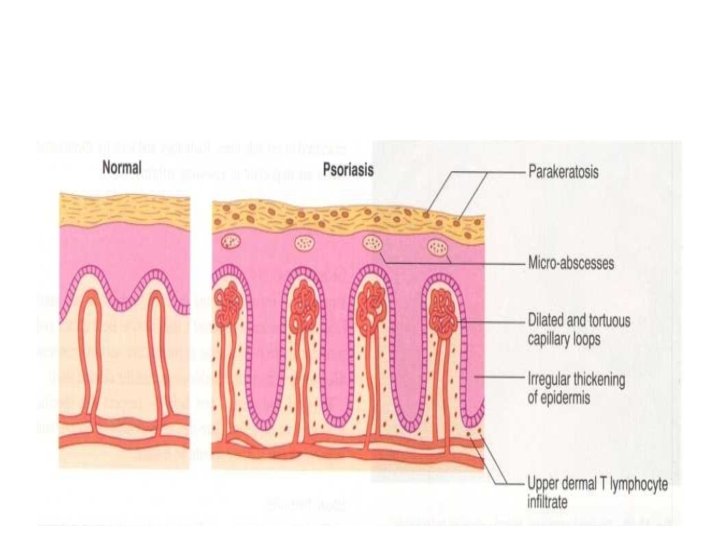
Histology The main changes are the following 1. Parakeratosis (nuclei retained in the horny layer 2. Irregular thickening of the epidermis over the rete ridges, but thinning over dermal papillae. 3. Epidermal polymorphonuclear leucocyte infiltrates and micro-abscesses. 4. Dilated and tortuous capillary loops in the dermal papillae. 5. T-lymphocyte infiltrate in upper dermis.

Clinical pictures Plaque pattern This is the most common type. Lesions are well demarcated and range from a few millimetres to many centimetres in diameter. The lesions are pink or red with large, centrally adherent, silverywhite, polygonal scales.


• Guttate psoriasis: lesions are the size of drops of water (may follow acute streptococcal infection). This is usually seen in children and adolescents

Psoriasis of the scalp discoid lesions or band-like plaque along the anterior hair line. predilection to frontal scalp margin are suggestive of psoriasis Significant hair loss is rare.

• Flexural psoriasis: affects the flexures as submammary area, groins & axillae. Owing to continuous friction & moisture at these sites, lesions are usually devoid of scales. Itching is a common symptom.
 • Involvement of the nails is common, with Pitting, onycholysis (separation of")
Nails(25 -50%) • Involvement of the nails is common, with Pitting, onycholysis (separation of the nail from the nail bed) and sometimes subungual hyperkeratosis, splinter-hemorrhage & circular areas of discoloration of nail bed & hyponychium “oil drop below nail.


Palms and soles • Palmar psoriasis may be hard to recognize, as its lesions are often poorly demarcated and barely erythematous. The fingers may develop painful fissures. Psoriasis of palm is differentiated from eczema by sharp margination at the wrist. • At other times lesions are inflamed and studdedwith 1– 2 mm pustules (palmoplantar pustulosis) The pustulosis are followed by brown macules or scales. often painful • Psoriasis of the palms and soles may be disabling.


Acute generalized pustular psoriasis This is a rare but serious condition, with fever and recurrent episodes of pustulation within areas of erythema.

Erythrodermic psoriasis This is also rare and can be sparked off by the irritant effect of tar or dithranol, by a drug eruption or by the withdrawal of potent topical or systemic steroids. The skin becomes universally and uniformly red with variable scaling. Malaise is accompanied by shivering and the skin feels hot and uncomfortable.


• • • Psoriasis is non-itchy Itching occurs in: Flexural psoriasis. Pyschogenic. Irritation of topical agents.

Psoriatic arthropathy Arthritis occurs in about 5– 20% of psoriatics. . Several patterns are recognized: • 1. Mono and asymmetric oligoarticular arthritis affecting proximal and distal inter-phalangeal joints sausage digit (the most prevalent type 70%). • Symmetric rheumatoid-like polyarthritis affecting proximal finger joints (-ve for RF). • Distal interphalangeal arthritis (Classic but uncommon). • Arthritis mutilans. • Spondylitis and sacroiliitis.


Differential diagnosis • • • Discoid eczema Seborrhoeic eczema Pityriasis rosea Secondary syphilis Cutaneous T-cell lymphoma Tinea unguium

Treatment • General measures • Explanations and reassurances must be geared to the patient’s or the parent’s intelligence. • The disease is not contagious. • In the end, the treatment is chosen by patient and doctor together after an informed and frank discussion of treatment options, including risks, mess, cost, compliance and co-morbidities.

• At present there is no cure for psoriasis; all treatments are suppressive and aimed at either inducing a remission or making the condition more tolerable. • However, spontaneous remissions will occur in 50%of patients
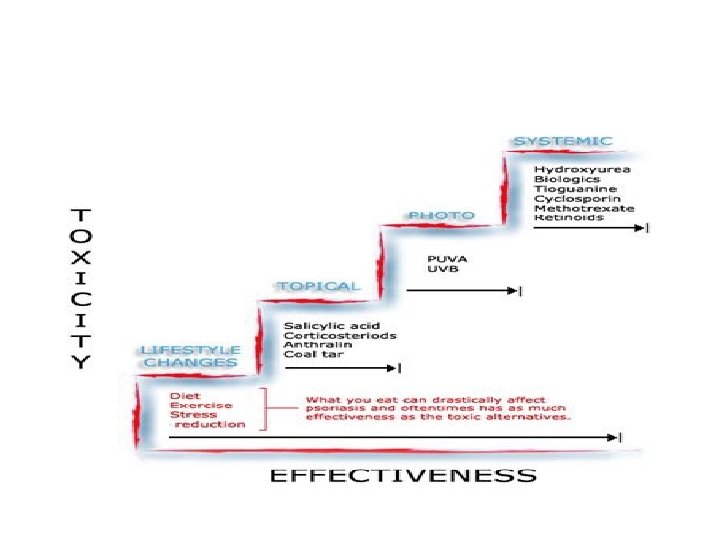

• Topical: as monotherapy in mild & localized cases and in combination in severe psoriasis. • Topical CS: 1 st-line treatment as monotherapy or in combination. • Calcipotriol (Daivonex®) oint. : 1 st-line treatment as monotherapy or in combination. • Dithranol 0. 1 -1. 0% paste: 2 nd-line treatment. • Tazarotene. • Salicylic a. 3% oint. • Crude coal tar oint. 2%.
 and PUVA or photochemotherapy")
• Phototherapy • UVB, narrow-band UVB (311 -313 nm) and PUVA or photochemotherapy (psoralen then exspose the skin to long wave UVA )as mono-therapy or in combination.

• Systemic therapy: in extensive cases or psychologically distressful patients • Methotrexate 7. 5 -30 mg in weekly oral divided doses at 12 hrs intervals for 3 doses each wk. It is effective but hepatotoxic. • Acitretin (Neo-tigason®) 1 mg/kg/day mainly in pustular & erythrodermic ps. but teratogenic. • Cy. A: “Neoral®” 2. 5 mg/kg/day. It is a selective immunosuppressant but nephrotoxic.
. • 2. Targeting")
Biological agents • 1. Targeting pathogenic T-cells, e. g. Alefacept (Amevive®). • 2. Targeting T-cell activation, e. g. Efalizumab (Raptiva®) and Alefacept (Amevive®). • 3. Anti-TNF , e. g. Etanercept (Enbrel®), Infliximab (Remicade®).


- Slides: 38