University of Minnesota Information Technology in Healthcare Course






























- Slides: 31
University of Minnesota Information Technology in Healthcare Course: MILI/PUBH 6562 Fall Semester B, 2005
Economic Valuation of Heath-care Fraud Under Different Electronic Health Record Scenarios Could Interoperability Drive Fraud? Stephen T. Parente, Ph. D. , M. P. H. , M. S. Director, Medical Industry Leadership Institute Karen Mandelbaum, MHA, JD Tilton & Dunn, P. L. L. P, Attorneys at Law December, 2009
Presentation Overview o Priors established from Brailler meeting. n Valuing non-credence goods n Look for detection in digital & physical worlds n Compare NHIN scenarios to status quo o o Economic model approach Preliminary economic model results Implications & caveats Next steps
Economic Valuation of Anti-Fraud Priors o Literature on anti-fraud valuation is largely driven by return on investment analyses by the anti-fraud industry and government reports. o Most analyses are before/after, with few controls. o Too diffuse a problem for economically efficient randomized controlled trials. o No seminal study to update, and even if so, the system-wide impact of interoperability is not yet known.
From Previous Economic Analyses on Fraud We Decided to Focus Primarily on Non-Credence Goods o Darby & Karni (1973), Free Competition and the Optimal Amount of Fraud, Journal of Law & Economics 16(1): 67 -88. n Distinguish three qualities of a ‘good’ sold in the market: o Search value (e. g. , I found this new doctor on the Internet. ) o Experience value (e. g. , The doctor saw me and I’m better now. ) o Credence value (e. g. , I like this doctor because she only prescribes brand name drugs). n Credence value, as a contributor to fraud (in the form of possible unnecessary care), is costly to value. n The regulation of such credence goods may be as expensive if not higher in marginal cost than the actual expenditure for the good.
Likely Non-credence Fraud Economic Issues for Health Interoperability o Potential Costs n Faster, more automated system means less chances of intervention. n If identity theft is the key to a robust fraud scheme, a national ID can open new gateways for this data. o Potential Benefits n More data to detect fraud patterns than before. o Real time patient data must come from same area. o IDs only from card swipes could be processed. Health benefit cards become tokens. o Marriage of ‘mature’ anti-fraud activities from credit cards ties to health benefits (e. g. , United Health Group’s Exante Bank/HSAs/Master. Card partnership). o Patient verification of diagnosis codes & charges could follow credit card consumer protection model. n Only realized with tailored decision support services.
Non-credence Fraud Economic Effects in Health Care as Related to IT Insurance related o Faked claims: affects profitability/surplus o Stolen identities: faked claim jet fuel – affects profitability Medical Care related o Faked goods (e. g. , DME): affects productivity and consumer welfare o Faked services: affects productivity and consumer welfare Regulator related o Inaccurate intervention: regulatory tax reduces consumer welfare, particularly if a ‘dynamic game’ by tipping one’s hand. o Imprecise intervention: regulatory tax reduces consumer welfare – found iceberg, didn’t probe beneath surface.
FRAUD We also decided to focus on fraud detectable in both the digital and physical worlds with a recognition that the digital world may be cracked depending upon the success of intelligent and analysis tools.
When you think about valuing anti-fraud activities, think of the Internet in the diagrams as automated surveillance, the physical market as the non-digital health care market and the pentagon as fraud activities. Some info of value It’s there but you can’t get it. It’s there, but not enough to care Digital surveillance gives you some, but not all of the picture.
Where We Started: Identify Fraud Pathways & Assign a Value & Probability to Them o Prior health care fraud valuations focus on the status quo. o These values ‘represent’ behavior information pathways of consumer, providers, insurers, and organized fraud enterprises. o Fraud in an interoperability needs to be valued as ‘treatment case’ to the status quo control.
Actual e. Links <90% Income Federal Government Courts Insurers To Build for Interoperability Congress Physicians Main Street Biotechnology Big Business 99% Income Hospitals 91 -99% Income
Assumptions – Four States of the World o W 1: Status quo without interoperability o W 2: Early NHIN with limited interoperability o W 3: Interoperability with intelligent coding tools o W 4: Interoperability with analytic tools to detect cyber fraud
What are Interoperability Standards? o Rapid implementation of interoperable EHR systems to exchange patient information required to deliver quality care as patients move from one care setting to the next. o Standards that can be updated incrementally to minimize both rework and costs as EHRs evolve to meet changing functional and environmental requirements.
What is Meaningful Use? o o The American Recovery and Reinvestment Act of 2009 authorizes the Centers for Medicare & Medicaid Services (CMS) to provide reimbursement incentives for eligible professionals and hospitals who are successful in becoming “meaningful users” of certified electronic health record (EHR) technology. These incentive payments begin in 2011 and gradually decrease. Starting in 2015, providers are expected to have adopted and be actively utilizing a certified EHR in compliance with the “meaningful use” definition or they will be subject to financial penalties under Medicare. CMS will be working closely with the Office of the National Coordinator for Health IT and other parts of HHS to develop regulations that will govern the initial year of the incentives programs, including a definition of meaningful use for 2011. The proposed rule, with a 60 -day period for public comment, is targeted for publication in late 2009.
An Interoperable Roadmap o Phase 1 – patient medical summaries to be fully specified in 2011. The definition of this first level of interoperability using the Integrating the Healthcare Enterprise (IHE) process (www. ihe. net) in the context of a new IHE Patient Care Coordination domain where clinician involvement is required. o Phase 2 – more coded clinical content for decision support, compatible with Phase 1, in 2011. This mid-level strategy focuses on a more refined coding of clinical information to support the convergence of the proposed new standards and the existing HL 7 CDA standard. o Additional phases to be defined as clinical practice and interoperability requirements evolve.
Valuing of Anti-fraud Activities as Cost. Benefit Analysis of Interoperability o Costs in W 1 through W 4 n Fraud Costs n Surveillance costs n Intervention costs n Non-Fraud Costs o Capital Costs of NHIN o Operating Costs of NHIN o Benefits in W 1 through W 4 n Fraud-Related o Reduced identify theft & verification of fake services n Non-Fraud Related o Reduced medical errors – consumer surplus from NHIN o Improved health status – consumer surplus from NHIN
Valuing of Anti-fraud Activities - Method o Inventory costs and benefits o Try to avoid double entry – this will undervalue benefit of fraud because a resource previously used for a fake care could be re-used to generate new value to a patient and society. o Create a spreadsheet model where costs and benefits were scaled at a national level. o Use existing literature where possible to inform: n Unit valuation (e. g. , hospital cost for EHR) n Probability fraudulent event n Likely change under different scenarios o When existing literature did not exist n Conservative starting point n Discussion with workgroup members and staff
Use of References & Assumptions for Unit Costs
Estimating Predicted Changes Under the 4 Different Scenarios
Costs – Fraud Related
Costs – Not-Fraud Related
Benefits –Fraud Related
Benefits – Not-Fraud Related
Cost/Benefits – Summary
Implications o Status Quo and Early EHR are expensive states. n Most of the assumed extra cost comes from new Medicare Part D fraud opportunities. o Interoperability (Scenarios #3 and #4) is cost saving and welfare improving for fraud related costs and benefits. o Interoperability can pay for itself.
Caveats o Model is best for framing costs and benefits. o Results will be more robust as trust in inputs is imparted either by clinical literature on expert opinion. o Model is not dynamic. Assumes extrapolating a 2005 -2009 expenditure to 2005 priors. o Presuming IT costs go down in terms of data storage, costs could be overestimated. However, IT costs are frequently overestimated in health IT projects (particularly involving clinical settings).
Small Group Exercise o Class Divides into Six Groups n n n American Hospital Association United Healthcare Mc. Kesson Medicare & Medicaid Department of Justice Tony & Junior Soprano o What is your group’s interaction with fraud & abuse activities? o Question to Answer: How will Hi. TECH and Meaningful Use Effect You?
EPILOGUE
If Jay Rockefeller and John Mc. Cain are in the same room, where might they agree? o Reduce Medicare ‘Waste, Fraud & Abuse’ n Waste: Defensive medicine n Fraud: Dead doctors billing for services n Abuse: Overutilization – legal use of services, but wasterful. o All 5 Bills have WFA in them o Questions: n Can it go from $5 -10 billion a year recovery to $50 billion? n Will DHHS/CMS allow a more aggressive strategy?
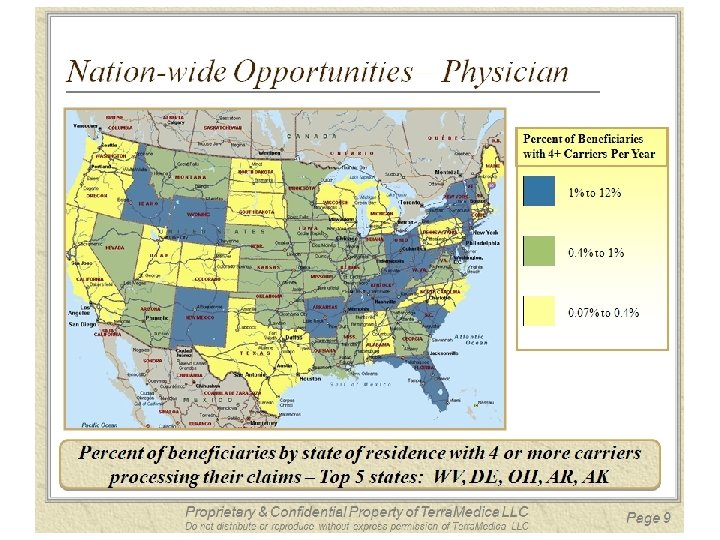
National CMS Level New Ideas Three example ‘opportunities’ to be scored: Suspicious claims submitted on behalf of a patient to 4 non-contiguous carriers Specialty specific patient illness burden to provider billed RVU ratio to systematically identify upcoding Combined with financial services external information – Goal – Score Transactions for Fraud Probability at Enterprise Level Proprietary & Confidential Property of Terra. Medica LLC Do not distribute or reproduce without express permission of Terra. Medica LLC Page 30