TUMOURS OF MIDDLE EAR AND MASTOID DR SUDEEP

Primary Tumours: Benign Glomus tumour Malignant Carcinoma , sarcoma 2)Secondary Tumours: a) From")

. � Females>Males. �")
Glomus jugulare: They arise from dome of jugular bulb,")
When tumour is intratympanic: Earliest symptoms are deafness and tinnitus. Deafness")

CT scan head 2)MRI 3)Four vessel angiography TREATMENT: Ø Surgical removal Ø Radiation")




- Slides: 15
TUMOURS OF MIDDLE EAR AND MASTOID DR. SUDEEP K. C.
CLASSIFICATION 1)Primary Tumours: Benign Glomus tumour Malignant Carcinoma , sarcoma 2)Secondary Tumours: a) From adjacent areas like nasopharynx , external meatus and parotid. b)Metastatic eg. From ca of bronchus, breast, thyroid, prostrate, GIT.
GLOMUS TUMOUR: � Most common benign neoplasm of middle ear and originate from the glomus bodies. It is found in the jugular bulb or on the promontory along course of tympanic branch of IXth cranial nerve(jacobson’s nerve). � The tumour consists of paraganglionic cells derived from the neural crest.
AETIOLOGY AND PATHOLOGY � Often seen in middle age. (40 -50). � Females>Males. � It is a benign non encapsulated but extremely vascular , slow growing and locally invasive tumours. � Microscopically it shows sheets of epithelial cells with large nuclei and granular cytoplasm with thin walled blood sinusoids without contractile muscle coat.
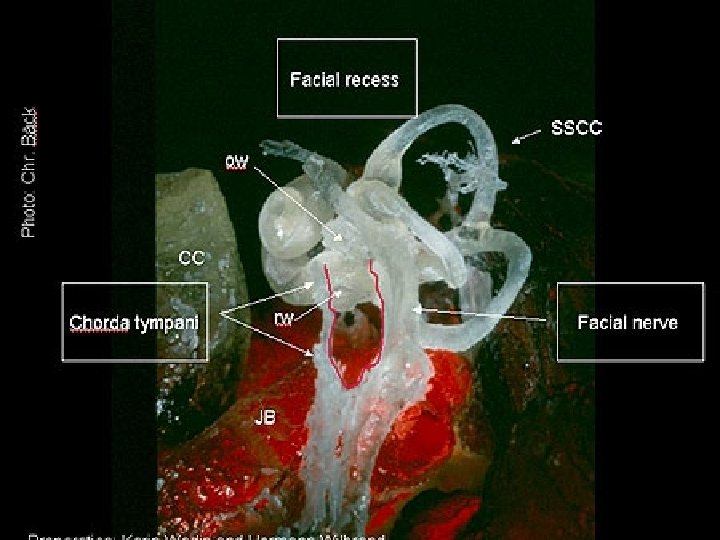
Two types of glomus tumours: 1)Glomus jugulare: They arise from dome of jugular bulb, invade hypotympanum and jugular foramen , causing neurological sign of IX th to XII th cranial nerve involvement. They may compress or invade lumen of jugular vein. 2)Glomus Tympanicum: They arise from promontory of middle ear and cause aural symptoms sometimes with facial paralysis.
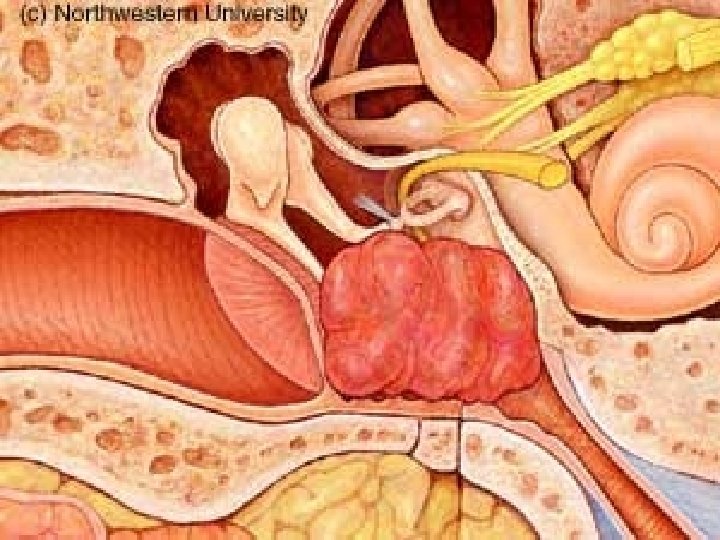
CLINICAL FEATURES: � A)When tumour is intratympanic: Earliest symptoms are deafness and tinnitus. Deafness is conductive type and tinnitus is pulsatile. Otoscopy show red reflex through intact TM. “Rising sun”appearance is seen. “Pulsation sign”(Brown’s sign) is positive. B) When tumour present as polyp: profuse bleeding from ear either spontaneously or after cleaning. Dizziness or vertigo and facial paralysis may appear. Earache less common otorrhoea due to secondary infection. Examionation reveals red vascular polyp.
Cranial nerve palsies: It is a late feature. IX th to XII cranial nerves may be involved. dysphagia , hoarsness with unilateral paralysis of soft palate, pharynx and vocal cord. � Tumours may present as mass over mastoid or in nasopharynx. � Audible bruit over mastoid. � Some glomus tumours secrete catecholamines and produce their symptoms. � Rule of 10 s: �
DIAGNOSIS: 1)CT scan head 2)MRI 3)Four vessel angiography TREATMENT: Ø Surgical removal Ø Radiation Ø Embolisation Ø Combination of the above techniques
CARCINOMA OF MIDDLE EAR AND MASTOID AETIOLOGY: Age- 40 to 60, females>males, chronic irritation may be the cause. PATHOLOGY: Tumour may arise primarily from middle ear or be an extension of ca of deep meatus. Squamous cell variety is most common.
CLINICAL FEATURES: Ø CHRONIC FOUL SMELLING DISCHARGE SPECIALLY BLOOD STAINED. Ø PAIN USUALLY SEVER AND COMES AT NIGHT Ø FACIAL PALSY Ø FRIABLE HAEMORRHAGIC GRANULATIONS OR POLYP Ø APPEARANCE OF OR INCREASE IN DEAFNESS OR VERTIGO.
DIAGNOSIS � DEFINITIVE DIAGNOSIS IS MADE ONLY ON BIOPSY � EXTENT OF DISEASE IS JUDGED BY CLINICAL AND RADIOLOGICAL EXMINATION. � CT SCAN & ANGIOGRAPHY ARE USEFUL IN THE ASSESSMENT OF DISEASE.
TREATMENT: � Combination of surgery and radiotherapy gives better results.