Integrating Interconception Care ICC into the Family Health
 into the Family Health Center of Worcester’s Early Well Child")
 and the goals")

 is the #1 cause of")











- Slides: 16
Integrating Interconception Care (ICC) into the Family Health Center of Worcester’s Early Well Child Visits Virginia Van Duyne, MD, Sara Shields, MD and Navid Roder, MD
Objectives Participants will be able to: • Describe Interconception Care (ICC) and the goals of integrating ICC screening into well child visits. • Understand how continuous quality improvement techniques can be used to create real process change in the implementation of ICC screening.
What is Interconception Care? • An emerging concept for focusing on the health of a woman from the postpartum period up until her subsequent conception • Family physicians are perfectly poised to do this (dyad care)
Why Interconception Care? • Preterm birth (PTB, <37 wks) is the #1 cause of neonatal mortality & morbidity • Low birthweight (LBW, <2500 g) is being linked to adult morbidities • Emerging studies link depression, short interpregnancy interval to these risks • 50% of smokers who quit in pregnancy relapse within 6 months postpartum (CDC)
What do we do in ICC? • Target modifiable risk factors: – Smoking – Depression – Folate supplementation – Lack of contraception • Integrate ICC into well child visits • Collect data using CQI – IMPLICIT network
Process Change • IHI Model for Improvement – Plan Do Study Act cycles – From Pilot to Implementation – Process!
Done by MA
Positive Screen No Folate Smoking Lack of Contraception Counsel on why folate 5 A’s: ask, advise, assess, assist, arrange Counsel on options Create encounter for mom: MA brings name, DOB to scheduler Wants prescription or referral? No *Document in child’s chart under Assessment (V 65. 40), copy & paste “Pos Screen for ___” from Template saved to desktop, fill in blanks Routine well child care Notify OB advocate and schedule follow up with PCP Place paper questionnaire in folder in resident office Ye s Depressed (PHQ 2 positive) Routine well child care while await mom’s registration Open mom’s chart (name is on questionnaire) Open mom’s chart , create Office Visit Create Prescription/ Referral Complete PHQ 9. Suicidal? No Create Prescription/ Referral Complete note in mom’s chart AND document in child’s chart under Assessment (see *) Ye s Get Soc Services involved, refer to EMH
Real Process Change
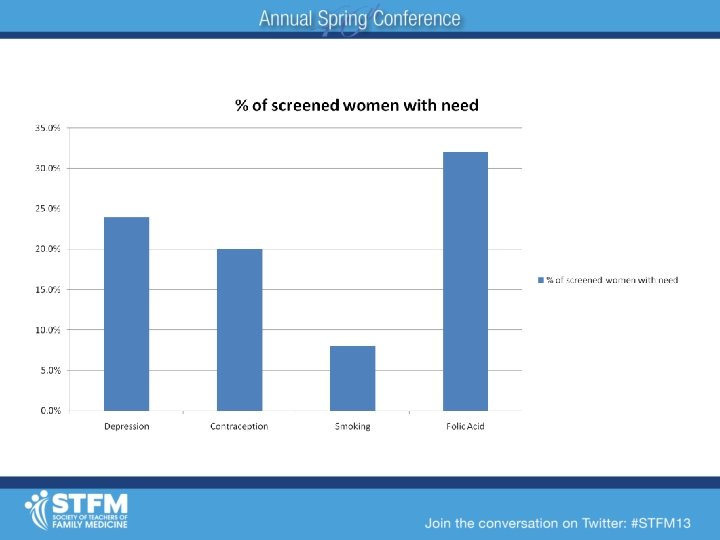
What we found… • 59% of the 34 screens done were positive for 1+ risk factor • #1 most common risk factor identified: Lack of vitamins (59%) • #2: Lack of contraception (25%)
What we found… • Depression and smoking had high rates of recurrence in the interconception period – Depression: 43% (n=7) – Smoking: 75% (n=4)
Ongoing work • One part time provider Oct 2012 Feb 2013 • 43 well child visits age 2 and under • 15 with ICC screening done (35%) – Another 10 with mom visit at same time (group or other)— 25 total (58%) • 13/25 (52%) of moms had an ICC need identified
Next steps • Restart ICC screening on a regular basis in provider’s practice • Implement ICC screening on clinic wide basis and track data • Assess clinical outcomes and develop interventions
Discussion • Any comments or questions? • Anyone here working on ICC in their health center? If so, how is it going? Specifically any comments on how you have integrated such specific screening into your EHR?
Bibliography • • • Brown & Eisenberg. Best of Intentions. National Academy Press: Washington, D. C. , 1995. CDC 2006 report Unintended Pregnancy Prevention Reproductive Health http: //www. cdc. gov/reproductivehealth/unintendedpregnancy/ date accessed: 4/16/2012 CDC –Tobacco Use in Pregnancy. http: //www. cdc. gov/reproductivehealth/tobaccousepregnancy/ accessed 4/21/2013. Conde Agudelo A, José M Belizán. Maternal morbidity and mortality associated with interpregnancy interval: cross sectional study. BMJ 2000; 321: 1255– 9 Conde Agudelo, et al. Birth spacing and risk of adverse perinatal outcomes: a meta analysis. JAMA 2006; 295: 1809 23. Downs DS et al. Design of the Central Pennsylvania Women's Health Study (Ce. PAWHS) strong healthy women intervention: improving preconceptional health. 2009 Jan; 13(1): 18 28. Epub 2008 Feb 13. Effects and safety of periconceptional folate supplementation for preventing birth defects. De Regil LM, Fernández Gaxiola AC, Dowswell T, Peña Rosas JP. Cochrane Database Syst Rev. 2010 Oct 6; (10): CD 007950. Review. Lumley J, Oliver S, Waters E. Interventions for promoting smoking cessation during pregnancy. The Cochrane Database for Systematic Reviews. Volume (3), 2004. Orr, et al. Unintended pregnancy and preterm birth. Paediatric and Perinatal Epidemiology 2000; 14: 309 313. Villar, J. , Merialdi, M. , Gulmezoglu, A. M. , Abalos, E. , Carroli, G. , Kulier, R. & de Onis, M. (2003) Nutritional interventions during pregnancy for the prevention or treatment of maternal morbidity and preterm delivery. An overview of randomized controlled trials. J. Nutr. 133: 1606 S– 1625 S.