OUR ROAD TO PCMH RECOGNITION Baldwin Family Health

OUR ROAD TO PCMH RECOGNITION Baldwin Family Health Care

Russ Kolski RN • Strategic Projects Director • Background in • Quality Management • Safety and Compliance • Accreditation (Joint Commission / AAAHC) • Given Medical Home Responsibility in July 2011 • PCMH Accreditation • Meaningful Use • Pay for Performance (Not my only role)

Baldwin Family Health Care • Health Center since 1967 • Rural Area • Serve West Central Michigan • 5 Medical Locations • 3 Locations with Retail Pharmacies • 3 School Based Health Centers • 25, 000 Annual Medical Visits • PCMH Status as of 2011 • AAAHC Recognized for PCMH • BCBS Recognized for PCMH at 2 of 5 locations

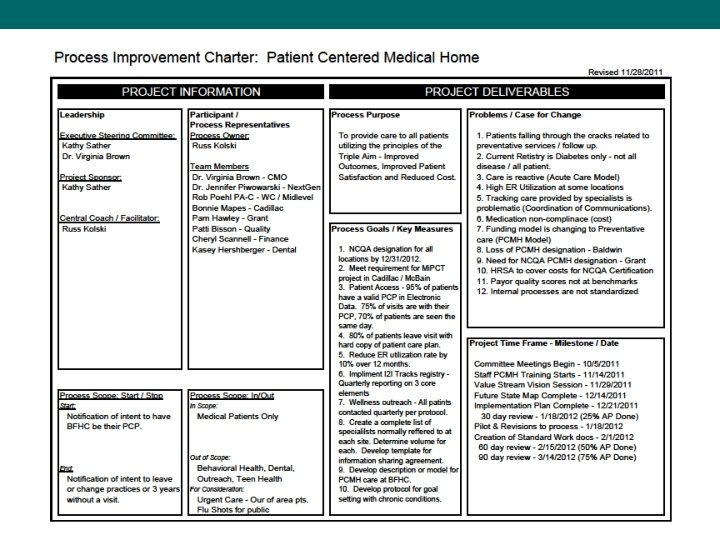
Baldwin Family Health Care Referral Tracking Pre-Visit Planning Dedicated Lead Annual Training PCMH Weekly HRSA Quality NCQA PCMH Mi. PCT / CMS First Site Live Last Site Live HRSA PCMH Staff Training Mi. PCT Case Implemented Hired Added Participation Transition to LEAN Event Implemented Submitted Education Trial Staff Road to PCMH Report Development Registry Enhancement Moved to Registry i 2 i Tracks Registry Huddles/Pre-plan Submission Pt. 2 Steering Comm. Submission Pt. 1 Managers Hired (Familiarization) Staff Work Flow Demonstration PCMH Module Next. Gen EHR NCQA PCMH Open Access Quality Dept. for All Patients Quality Staff MU Stage 2 Workgroup MU Year 1 Selected Funding in ACO Oct. 2012 – Feb. 2013 September 2011 September 2012 November 2011 December 2011 November 2012 December 2013 February 2013 January 2012 October 2011 Started 2011 August 2012 January 2012 June 2011 June 2012 June 2013 March 2012 April 2012 May 2012 July 2012

“IF WE KEEP DOING WHAT WE ARE DOING, WE WILL KEEP GETTING WHAT WE GOT. ” Yogi Berra

Personal PCMH Learning • Limited Understanding at Start • Attended PCMH Seminars • Local PHO • Michigan State Medical Society • Obtained Chronic Care Professional Certification • Reading • • LEAN – Toyota Production System Transfor. Med IHI PATH
 •")
Internal Planning • EHR Transition (1 st site live 12/2011 – last 6/2012) • Provider Coordinating Committee • Transition Committee • Established PCMH Steering Committee • Education at all levels • Visit Workflow Re-design • Transition from Acute Care to Preventative / Wellness Based Care • Match pre-EHR Provider Productivity • Integrate PCMH Elements into Standard Work
 • PCMH Lead • Quality Manager • Chief")
Steering Committee Membership • CEO (Ex-Officio) • PCMH Lead • Quality Manager • Chief Medical Officer • Physician Lead for EHR • Mid-level Provider • COO / Privacy Officer • Site Facility Manager • Finance Representative • Dental Representative* • Behavioral Health*

“EVERY SYSTEM IS PERFECTLY DESIGNED TO GET THE RESULTS IT GETS. ” Paul B. Batalden MD Co-founder Institute for Healthcare Improvement Founding Director Center for Healthcare Improvement and Leadership – The Dartmouth Institute

New Structure • Eliminate Medical Support Specialist Role at 5 sites • Former Diabetes Registry Coordination (Old PECS System) • Centralize Registry Function within Quality Department • Added Quality Department Staff • PCMH Registry Specialist – May 2012 • PCMH Report Generator – May 2012 • Care Managers for 2 locations (Mi. PCT) – January 2012 • CMS Muliti-payer Demonstration Project • Create PCMH Lead at each site – May 2012 • Additional responsibility for selected staff member

Planning Tools • Annual Performance Improvement Plan • Schedule of Activities • Comparison of Clinical Quality Measures for UDS/MU/PCMH/Pay for Performance Measures • Crosswalk between NCQA and BCBS PCMH Standards • Working examples will be shown at end of presentation

Annual PI Plan Activity

Activity Schedule Clinical Quality Indicator Reporting January UDS ED Visits Open Access February March April May June July Record Audit MU UDS 7 Day post Hospitalization Generic Rx Rate ED Visits with PCP Patient Self Mgt. Open Access August Record Audit 7 Day post Hospitalization Visits with PCP September October November December UDS/MU PH Medications UDS MU Generic Rx Rate ED Visits 7 Day post Hospitalization Generic Rx Rate Patient Self Mgt. Open Access Visits with PCP Patient Self Mgt. Framework for Clinical Portion of Annual PI Plan Monthly Patient Contact Schedule January February March April May June July August September October November December Item 1 Diabetes HTN Asthma Item 2 Well Child - 7 -21 Well Child - Years / Lead Well Child - 3 to 6 Item 3 Immunizations 7 -12 Immunizations - 15 Mo Immunizations 3 - 6 Item 4 Chlamydia Pap/Mam Colonoscopy Item 5 Cardiovascular Osteoporosis / RA COPD Item 6 Smoking Cessation BMI Chronic Kidney

Periodic Assessment - BCBS

What Needs Measured?

Goal Comparisons

Periodic Assessment - NCQA

NCQA Report Priorities

Data Location and Reporting

NCQA Reporting

Evidenced Based Care - MQIC

Protocol Creation / Modification

Staff / Patient Tools • PCMH Brochure • Care Management / Self Management Documentation • Standardized Work Documentation • Staff Education Tools

PCMH Brochure

Care Planning

Create Staff Documentation

Success’ • Next. Gen EHR Implementation • i 2 i Tracks Registry Implementation • Centralized PCMH Functions • Mailings for all sites using fold and seal mailers • Report processing and distribution • One Time download of all immunization in State Immunization Registry (MCIR) to our EHR • PCMH Module in Annual Competency Training • Planning • Worked Smarter, not Harder • Made sure Measures met multiple goals
 • Open Access Scheduling • Competing Priorities • Internal CAHPS Surveying")
Weak Areas (Failures) • Open Access Scheduling • Competing Priorities • Internal CAHPS Surveying • Costly • Time Consuming • Interfaces • MCIR Upload • Identification of Managed Care Population • 4 different attempts • Too Large – Wrong Measures – Too Small – Just Right • Provider Engagement • Competing Priorities (Productivity / EHR / PCMH)
 • Provider • Staff (Clinical and")
Pearls • Education • Leadership (Administration and Board) • Provider • Staff (Clinical and Support) • Change is Difficult • Changing to the Chronic Care Model is More Difficult than meeting the NCQA PCMH Standards • Staff and Providers do not want to give up the old way • Competing Priorities • Care Management Population Selection • What is your time frame to meet goal? – Work Backwards • What percent of your proposed patients are seen during that time? • Who will do Care Magement?

Pearls • Registry • • Data Validation How will you measure various aspects of care? Will your registry report on those items? Success is tied to staff proficiency with EHR. • Standardize • What will be documented where? • Who will perform specific ongoing reporting tasks? • Adopt the “Everyone works to their highest level of licensure or training” philosophy. • Live the “Triple Aim” and immerse yourself in PCMH

Pearls • Communication • Newsletters • Reference Materials for Staff • Investment • Financial (Registry / Licenses / Education / Staffing) • Staff Time (Education / New Tasks / Learning Curve) • Flexibility • Modify timeline as needed • Ask for help

Success? • NCQA PCMH Designation at all 5 sites • Meaningful Use Payments for Stage 2 (2014) • Reporting • Valid Results • Available for all known measures • Trending data available • Improved Quality Scores • UDS • Pay for Performance Indicators – All Payers • Gain Sharing with our new ACO Initiative
- Slides: 33