Groin swellingg Groin swelling History when the lump



: site ,")













")
- Slides: 23
Groin swellingg
Groin swelling History : • when the lump 1 st notice ? • what are the symptom related to lump? • Has lump change ? in size , shape , color since it was appear ? • Dose the lump ever disappear ? what makes the lump disappear ? • Has the patient had any ather lump ? • What dose the patient think cause the lump ? • Is there any discharge ? • What ttt has been suggested or administered ?
• Also we have to ask potential complication of hernia : 1. Irreducibility 2. Obstruction : abdo pain , distension , constipation , vomiting 3. Strangulation : tender, painfull 4. • Also we ask about risk factor for hernia : 1. Chronic cough 2. B. A 3. Chronic constipation 4. Straining with urination 5. Occupation • Social hx : smoking , occupation , heavy lifting
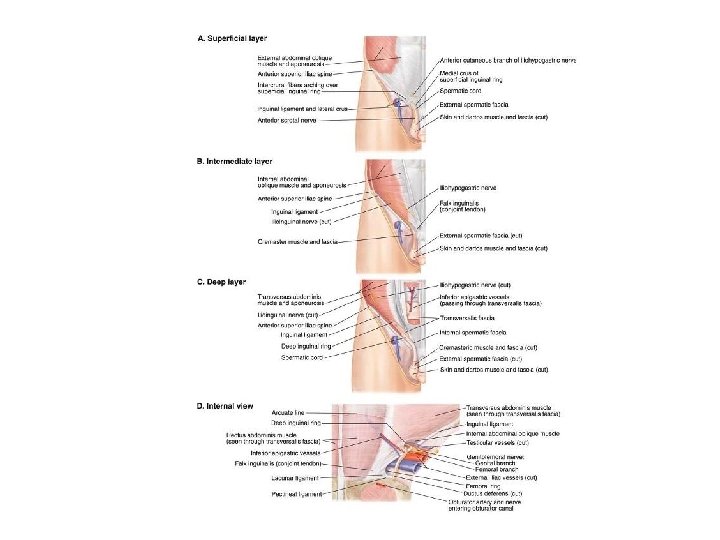
Examination: • Inspection , palpation , auscultation • Asymmetry ( swelling ): site , size , tenderness , mobility • Neck……. . defect • Sac…………content • Overlying skin • Reducibility Expansilecough
• Differential diagnosis of groin swelling : 1. Inguinal hernia 2. Femoral hernia 3. Femoral aneurysm 4. Lymphadenopathy 5. Ectopic testis undescending testis 6. Lipoma of spermatic cord 7. Hydrocele of cord 8. abcess
• For dx of swelling we have to do : 1. Ultra sound 2. CT abdomine 3. AXR erect + supine
• Hernia : is protrusion of viscus into an area in which it is not normally contained. • Male>femal = 9: 1 • Most common surgical disease of males.
• • Type of common hernia : Inguinal : 80% Umbilical : 15 % Femoral : 5 %
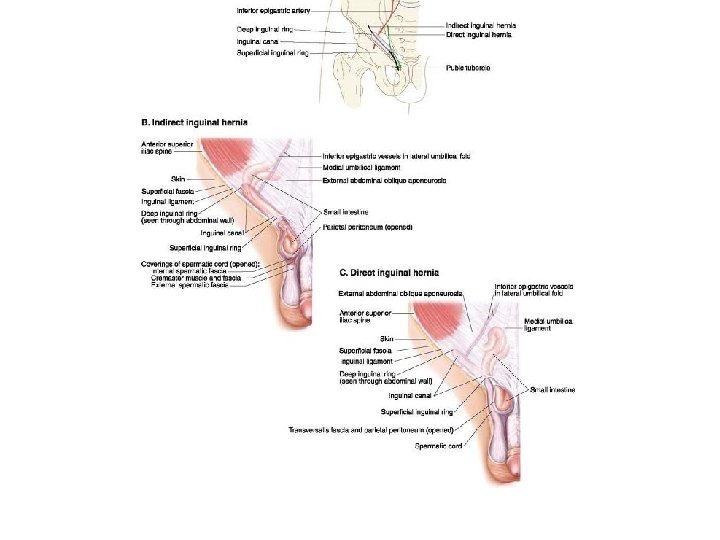
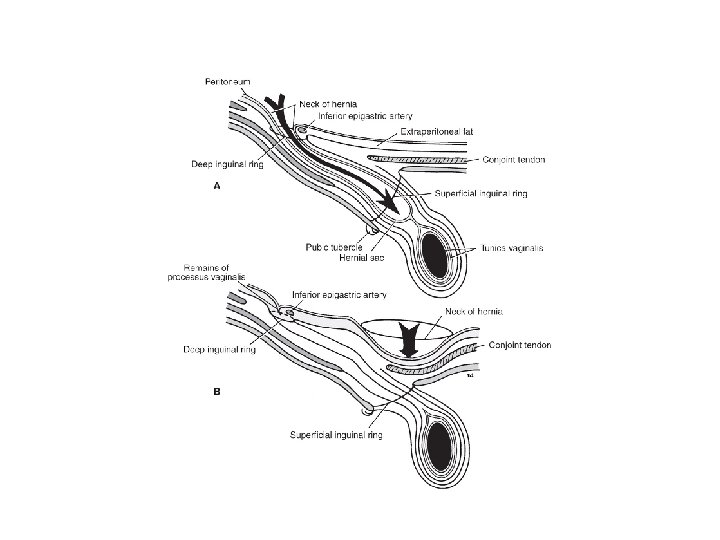
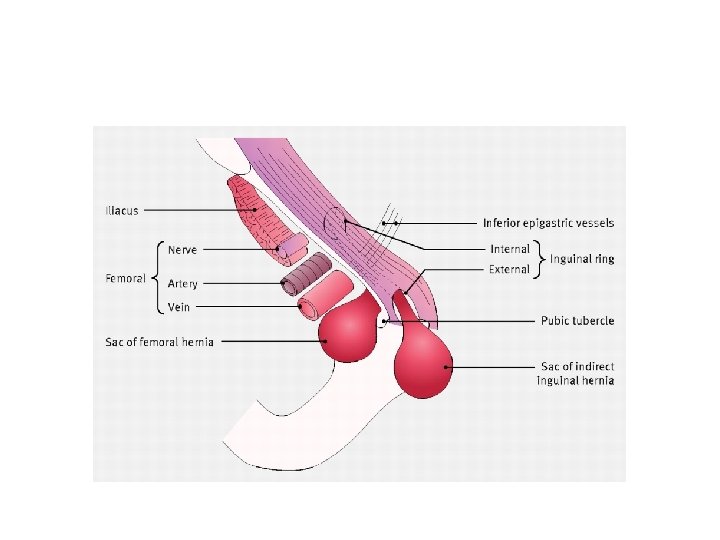
Inguinal hernia indirect Direct vs indirect • Originate at deep inguinal ring Directly through the abdominal pass to ext. inguinal ring wall muscle (hesselbach’s triangle ) Lateral to inferior epigastric vessel Medial to I. Epi. GAstric vessel More likely to be incarcerated Less likely to be in carcerated than indirect Pass to scrotal sac Usually not pass to scrotal Etiology : congenital Etiology : aquired weakness in persistence of processus transversalis fascia or increase vaginalis in 20% of adults intra-abdominal pressure All inguinal hernia reduced to point above and medial to pubic tubercle
Complication of hernia 1. Incarceration 2. Strangulation 3. Ischemia 4. Necrosis 5. Intestinal obstruction This complication need ergent surgery and laproscopic exploration
• Sign and symptom of peritonitis are absolut indication for abdominal exploration
Treatment • 1 - observation for asymptomatic small inginal hernia and reducible and repaired electively • 2 - can be reduced manually if no strangulation . how? • 3 - don’t attepmt to reduce hernial sac if sepsis or gangernous occure it is surgical emergency • 4 - surgical repaire for indirect : tension free mesh repaire
Treatment Surgical repaire for direct : bassini , Mcvay , lichtenstienrepaire Can be done open or laproscopic Laproscopic usefull for patient has recurrent or bilateral hernia.
Post -operative complication 1. 2. 3. 4. 5. 6. 7. Recurrence Scrotal hematoma Nerve entrepment Ischemia and occlusion of femoral vein Wound infection Temperary urinary retintion Injury to spermatic cord structure
Femoral hernia 1. Origin from femoral ring and pass to saphenous hiatus through femoral canal. 2. Pass medially to femoral vein artery nerve. 3. Occure mush more in women but still the inguinal is most common. 4. Prone to incarceration and strangulation 5. Point of reduction ( below and lateral to pubic tubercle )
Treatment • Femoral hernia are generally repaired because it is high risk for strangulation. • Reduction is often difficult • Is nessery to assure adequate closure of femoral canal
Hematoma • Blood collection within muscles layer of ant abdominal wall • Due to mild truma or blood disease • Present with abdominal pain and painfull abdominal mass and may be ecchymosis over abdomine • fothergill’s • Dx by CT + u/s • Usually resolve without surgery and evacuation done if clot with adequate hemostasis with sever pain and persistent
Tumar of abdominal wall • Mostly benign ( lipoma , hemangioma , fibroma ) • Rarly malignant and often from mets from intra-abdominal sourse