GOOD MORNING 37 year old female patient complains





. CLINICAL FEATURE Searing, stabbing, lancinating pain Older adults Females than")



 SLUDER’S HEADACHE/ VIDIAN NEURALGIA ETIOLOGY: Hypothalamic hormonal influences Genetic predisposition")

























- Slides: 37
GOOD MORNING!!!!!!
37 year old female patient complains of pain over the right side of the face. No dental complaints No carious tooth No periodontal problems
DISEASES OF NERVES
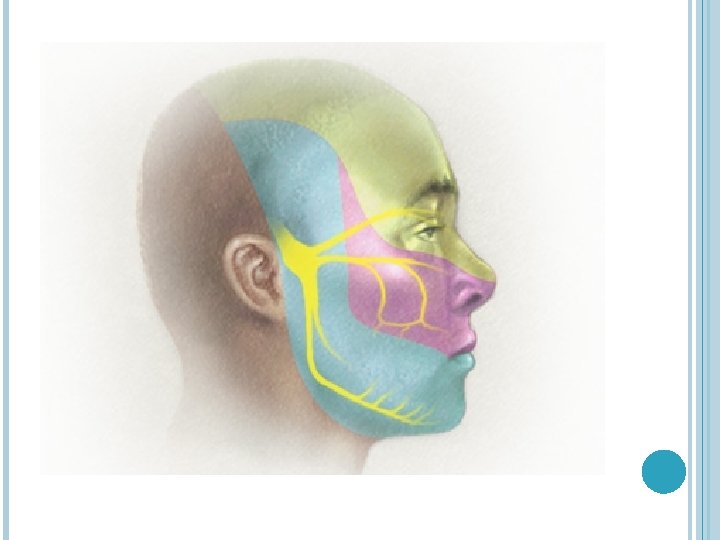
TRIGEMINAL NEURALGIA Tic Douloureux Trifacial neuralgia Fothergill’s disease History
TRIGEMINAL NEURALGIA Archetype of orofacial neuralgias Mainly affects 2 nd and 3 rddivision of the trigeminal nerve Paroxysms Always associated with ‘TRIGGER ZONES’
TRIGEMINAL NEURALGIA (TIC DOULOUREUX). CLINICAL FEATURE Searing, stabbing, lancinating pain Older adults Females than males Right side more common Trigger zones Pretrigeminal neuralgia Fear of attack Mostly unilateral
ETIOLOGY Mystery !!! Peripheral injury or disease of nerve Failure of central inhibitory mechanism. Compression of trigeminal roots by tumors or vascular anomalies Abnormal vessels Aneurysms Chronic meningeal inflammation With multiple sclerosis
TRIGEMINAL NEURALGIA Differential diagnosis Migrain Sinusitis Costen syndrome Tumors of the nasopharynx Trotter’s syndrome Postherpetic neuralgia Trigeminal neuritis
TRIGEMINAL NEURALGIA Investigations : MRI Treatment: Peripheral neurectomy Injection of alcohol Injection of boiling water Phenytoin sodium Carbamazepine Microsurgical decompression of trigeminal root
SPHENOPALATINE NEURALGIA (HORTON’S SYNDROME) SLUDER’S HEADACHE/ VIDIAN NEURALGIA ETIOLOGY: Hypothalamic hormonal influences Genetic predisposition
SPHENOPALATINE NEURALGIA CLINICAL FEATURES: Unilateral intense pain No ‘Trigger zone’ Sneezing, swelling of the nasal mucosa, severe nasal discharge Epiphora, bloodshot eyes Men commonly affected < 40 years “Alarm clock”
Treatment-alcohol injection, resection of the ganglion
BURNING MOUTH SYNDROME Postmenopausal females more common Multifactorial causes stress, nutritional deficiency, diabetes mellitus, sjogren’s syndrome. Clinical features Continuous or intermittent discomfort- frequently affecting tongue sudden or gradual over months associated with psychosomatic disorders, dry mouth
Treatment Antidepressants vitamins analgesic sprays hormone replacement saliva substitute.
AURICULOTEMPORAL SYNDROME ETIOLOGY: Damage to nerve-removal of parotid tumor or ramus of mandible or parotitis CLINICAL FEATURES: Flushing and sweating of involved site-temporal area common site Crocodile tears
STARCH- IODINE TEST
TREATMENT
GLOSSOPHARYNGIAL NEURALGIA Similar to trigeminal neuralgia CLINICAL FEATURES No gender prediliction Middle age or older persons Sharp, shooting pain in the ear, pharynx, nasopharynx, tonsil or posterior portion of the tongue TRIGGER ZONE-tonsillar fossa
ETIOLOGY-unknown, neural ischemia has suggested Treatment: Resection of the of nerve
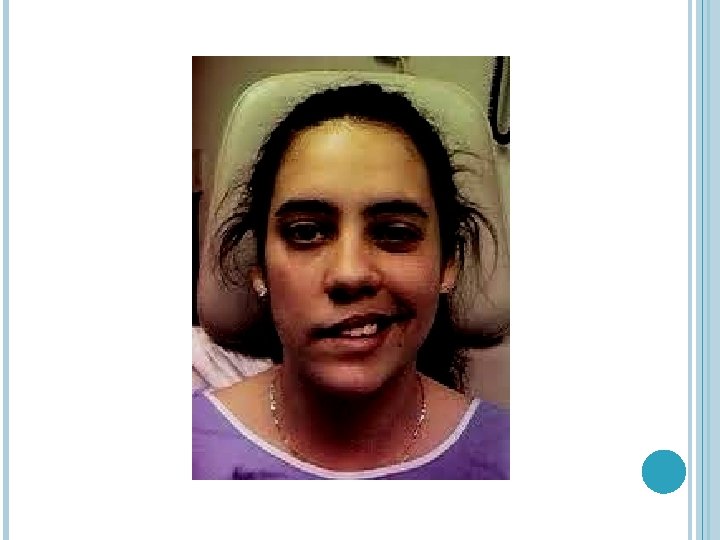
Julia awoke with a crooked smile she thought she had a stroke because she could not move the right side of her face no matter how hard she tried. Her eye would not close completely and she could not raise the corner of her mouth. Her grandfather had recently suffered a stroke and Julia worried that she also had a stroke because, in the mirror, her face looked like her grandfather's.
BELL’S PALSY Sir Charles Bell Etiology § herpes simplex infection § inflammation of the facial nerve § iatrogenic v v Melkerson - Rosenthal syndrome Ramsay Hunt Syndrome
CLINICAL FEATURES Unilateral usually Familial occurrence Females Middle age
CLINICAL FEATURES
? Can raise eyebrows, the facial nerve is intact. Woman has left side brain paralysis of the right lower face Man has right bell’s palsy,
TREATMENT No specific treatment Histamine Physiotherapy Try to prevent eye infection Synkinesis
ATYPICAL FACIAL PAIN Group of conditions, poorly localized pain in region of 2 nd , 3 rd , 5 th and 9 th cranial nerve Pain is unanatomic No trigger zone Severe as trigeminal neuralgia but different
ATYPICAL FACIAL PAIN ETIOLOGY Injury to T. N due to trauma Differential diagnosis: Trigeminal neuralgia Eagle’s syndrome(elongation of styloid process or ossification of stylohyoid ligament)
Treatmentless satisfactory than Trigeminal neuralgia non-narcotic drugs like tricyclic antidepressants phenytoin – intermediate effectiveness carbamazepine – least effective.
HORNER’S SYNDROME Sympathetic opthalmoplegia Miosis Ptosis Anhydrosis
MIGRAINE
CLINICAL FEATURES 2 nd decade Preheadache phenomenon Pain in temporal, frontal and retro-orbital areas.
TREATMENT Ergotamine Methylsergide
MARCUS GUNN PHENOMENON Trigemino-oculomotor synkinesis Congenital unilateral ptosis with rapid elevation of the ptotic eyelid occuring on movement of the mandible to contralateral side Jaw-winking syndrome Marin Amat syndrome