Community Acquired Pneumonia Is Penicillin Resistance Relevant Edward


















 2 gm po BID (with macrolide on admission) –")















. • Bratzler, D (Personal Communication")
- Slides: 44
Community Acquired Pneumonia: Is Penicillin Resistance Relevant? Edward L. Goodman, MD, FACP, FIDSA, FSHEA June 30, 2008
Basic Diagnostic Criteria • History – – Cough Fever Sputum production Pleurisy • Physical Exam – Altered breath sounds/percussion – Rales • Imaging: CXR (PA/Lat if possible); CT not usually required • Pulse Oximetry
Need For ICU Admission: 1 major or 3 minor criteria Mandell LA et al. IDSA/ATS Consensus Guidelines. Clin Inf Dis 2007; 44: S 27 -72
ID Society/ATS Practice Guidelines CID 2007; 44: S 45 • Recommended empirical antibiotics for community acquired pneumonia – Inpatients, non ICU treatment • A respiratory FQ (level 1) • A beta lactam plus a macrolide (level 1) – Inpatients, ICU treatment • A beta lactam (cefotaxime, ceftriaxone, amp/sulb) plus either azithromycin (level 2) or respiratory FQ (level 1) • For pen allergic, aztreonam and respiratory FQ – These Guidelines are the basis for CMS Scorecards • Failure to comply leads to diminished hospital reimbursement • Public reporting of compliance has started in 2008
Rationale for IDSA/ATS Guidelines • Increasing Penicillin resistance • Need for atypical coverage • Availability of FQs which – Are highly bioavailable – Cover atypicals – Are rapidly bactericidal
Why Add Macrolide to Beta Lactam? • To cover atypical pathogens which Beta Lactams don’t cover – Chlamydophilia – Mycoplasma – Legionella
Why Add Macrolides? • Added benefit beyond antimicrobial effects? – Several retrospective studies suggested better outcomes when macrolide added to beta lactam for bacteremic Pneumococcal pneumonia • Etiology not in doubt • Postulated immunomodulatory effect – Recent prospective study partially confirmed: • Baddour, Yu et al 2004
Am J Respir Crit Care Med 2004; 170: 440
Baddour L, Yu V et al. Combination Antibiotic Therapy Lower Mortality among Severely Ill Patients with Pneumococcal Bacteremia. Am J Resp Crit Care Med 2004; 170: 440
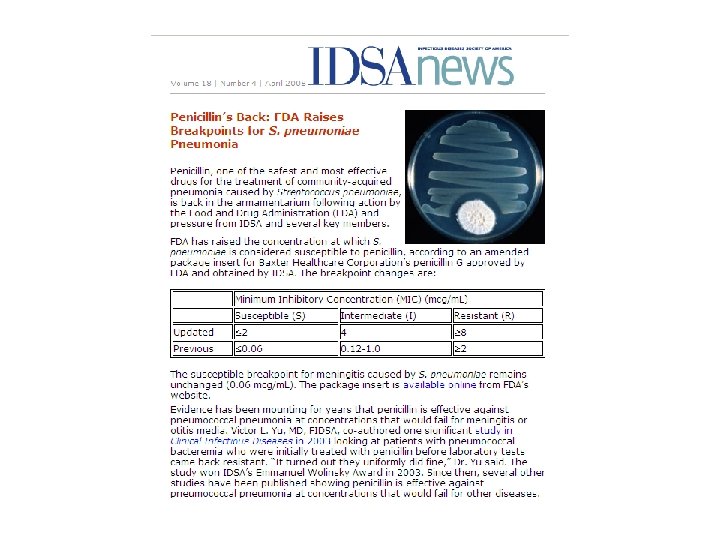
What About Increasing Resistance to Penicillin? • In 1968 we used Procaine Pen G 600, 000 IM BID for CAP (presumed pneumococcal pneumonia) • Much data on rising MIC’s for Strep pneumoniae – FQ’s activity not related to Pen “non susceptibility”
Distribution of Streptococcus pneumoniae Antimicrobial Resistance Across the US Erythromycin Penicillin Erythromycin- intermediate intermediat (MIC 0. 5 resistant (MIC e (MIC 0. 12 mg/L) ≥ 1 mg/L) – 1 mg/L) n Penicillinresistant (MIC ≥ 2 mg/L) NORTHWEST 422 17. 3% 10. 4% 23. 2% 0. 5% NORTHCENTRAL 2106 26. 3% 11. 3% 31. 7% 0. 1% NORTHEAST 3708 21. 7% 11. 5% 26. 5% 0. 3% SOUTHWEST 1349 27. 0% 15. 4% 29. 3% 0% SOUTHCENTRAL 1455 32. 5% 13. 8% 38. 6% 0. 3% SOUTHEAST 1063 36. 4% 14. 0% 40. 2% US Region Doern G et al. J Infect 2004; 48(1): 56 -65.
Net Effect • Every febrile patient in ED with the slightest abnormal CXR gets Levaquin or Avelox! – Heavily promoted by drug makers – IDSA Guidelines indirectly encourage it • Resistance to FQ rising at an alarming rate among E coli and Pseudomonas • Rising rates of C diff and MRSA can be attributed, in part, to FQ pressure
2004 Antibiogram PHD
2007 PHD
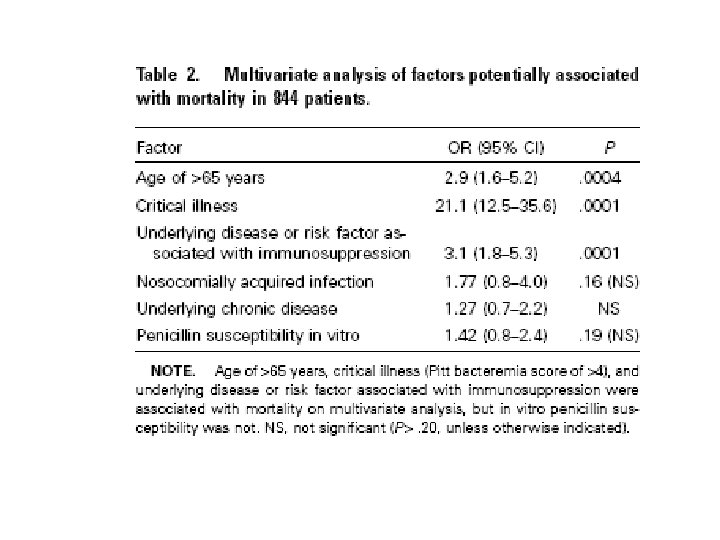
Is Penicillin Resistance Relevant in Treating CAP? • Clearly in Pneumococcal meningitis resistance is critical – Poor penetration into CSF by penicillin – Immunologically “privileged sanctuary” • No complement • Minimal immunoglobulin • Not relevant in pneumonia or bacteremia
Clinical Infectious Disease 2003; 37: 230
To Recap • IDSA/ATS Guidelines are basis for “scorecards” judging adequacy of therapy for CAP • These Guidelines “favor” monotherapy with Fluoroquinolones • FQ resistance and “collateral damage” rising • Penicillin “resistance” redefined – irrelevant for CAP and bacteremia
Solution? • Amoxicillin/clav (Augmentin XR) 2 gm po BID (with macrolide on admission) – ampicillin/sulbactam IV is included in IDSA/ATS guidelines • Amox/clav microbiologically equivalent for respiratory pathogens – Serum levels of 2 gm amox well above MIC for Strep pneumo • Therefore, less pressure to use FQ
Query to Dale Bratzler, DO CMS consultant 5/14/08 • For empiric Rx of non-ICU CAP, why not use po Amoxicillin/clavulanate XR (plus an oral macrolide) for those patients who could take an oral regimen? • For non-ICU CAP where the etiology is known with reasonable certainty, will specific therapy be a “fallout” if it is not in the IDSA/ATS Guidelines?
Responses from Dr. Bratzler • “With the exception of oral fluoroquinolones, oral antibiotics are not recommended for the treatment of hospitalized patients with pneumonia – at least not initial therapy. ” • “I am not sure of the exact bioavailability of Augmentin, but it is not recommended in the Guidelines and will not be in the pneumonia performance measure. ” • “I think this is a fine choice for an outpatient. I am not aware of studies of treatment of inpatient pneumonia with …. Augmentin. ”
Bratzler - continued • “…if a patient has a positive test for a pathogen (and the test result is available to the physician within the first 24 hours of admission), the case is excluded from the antibiotic selection performance measure. ”
Can We Refute Bratzler? • “I think this is a fine choice for an outpatient. I am not aware of studies of treatment of inpatient pneumonia with …. Augmentin”
Augmentin XR® Package Insert • Four randomized, controlled, double blind and one non comparative studies in adults with CAP • In comparative studies 904 patients • In non-comparative study 1122 patients • Dose: Amoxicillin 2 gm/clavulanate 125 mg po BID • Results: – Comparative: 86. 3% - 94. 7% clinical success – Non comparative: 85. 6% clinical success
Augmentin XR® Package Insert Clinically Evaluable with Reduced Susceptibility to Penicillin n/N MIC All Strep 275/297 pneumo MIC = 2 18/18 % 95% C. I. 92. 6% ---- 100% 81. 5 -100 MIC>2 24/25 96% 79. 6 -99. 9 MIC>=4 6/7 85. 7% 42. 1 -99. 6
Should I Appeal to CMS? Gustave Dore 1863 Don Quixote Tilting at Windmills
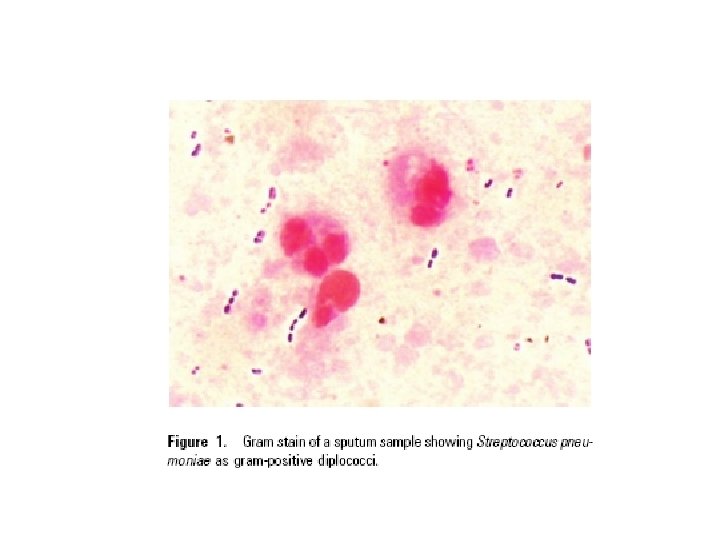
Rapid Detection of Etiology • “…if a patient has a positive test for a pathogen (and the test result is available to the physician within the first 24 hours of admission), the case is excluded from the antibiotic selection performance measure. ” – Excluded from report cards! – Less need for broad spectrum, empiric therapy – e. g. , fluoroquinolones • Only two current rapid diagnostic tests exist – Sputum gram stain – Urine Pneumococcal Antigen test
Musher DM et al. Diagnostic Value of Microscopic Examination of Gram -stained Sputum and Sputum Cultures in Patients with Bacteremia Pneumococcal Pneumonia. Clin Inf Dis 2004; 39: 165 -9
Musher. CID 2004; 39: 165 -9
Pneumococcal Urine Antigen • Sensitivity: 70 -80% • Specifity: >90% – False positives • In children • Recently vaccinated • Remains positive for several weeks
Conclusions • Urine Antigen on all cases of CAP – If positive • consider treatment with amoxicillin 1 gm po TID or IV ampicillin 1 gm Q 6 H • Not included in calculation of score cards – If negative • Follow IDSA Practice Guidelines • Obtain induced sputum for gram stain and culture – Lower sensitivity requires initial adherence to IDSA/ATS Guidelines – Allows potential for pathogen identification • allows sensitivity tests • Allows switch to narrow spectrum therapy – i. e. , amoxicillin
ID Society/ATS Practice Guidelines CID 2007; 44: S 45 • Recommended empirical antibiotics for community acquired pneumonia – Inpatients, non ICU treatment • A respiratory FQ (level 1) • A beta lactam plus a macrolide (level 1) – Inpatients, ICU treatment • A beta lactam (cefotaxime, ceftriaxone, amp/sulb) plus either azithromycin (level 2) or respiratory FQ (level 1) • For pen allergic, aztreonam and respiratory FQ
Bibliography • Baddour LM, Yu VL et al. Combination Antibiotic Therapy Lowers Mortality among Severely Ill Patients with Pneumococcal Bacteremia. Am J Resp Crit Med 2004; 170: 440. • Mandell LA, Wunderlink RG et al. Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community Acquired Pneumonia in Adults. Clin Infect Dis 2007; 44: S 27 -42.
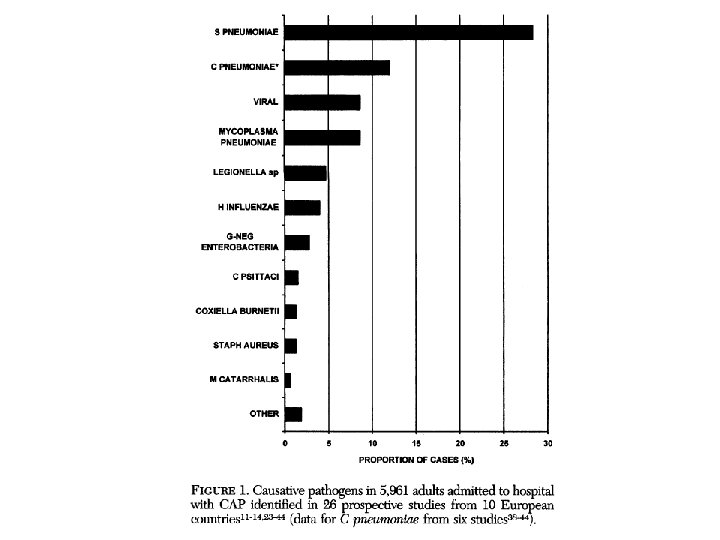
Bibliography • Musher DM, Montoya R, Wanahita, A. Diagnostic Value of Microscopic Examination of Gram. Stained Sputum and Sputum Cultures in Patients with Bacteremia Pneumococcal Pneumonia. Clin Infect Dis 2004; 39: 165. • Werno AM, Murdoch Dr. Laboratory Diagnosis of Invasive Pneumococcal Disease. Clin Infect Dis 2008; 46: 926. • Woodhead M. Community-Acquired Pneumonia Guidelines an International Comparison: A View from Europe. Chest 1998; 113: 183.
Bibliography • Williamson, S (Personal Communication May 15, 2008). • Bratzler, D (Personal Communication May 15, 2008)