Pneumonia Rand Alshayeb Pneumonia Pneumonia is as an

Pneumonia Rand Al-shayeb

Pneumonia • Pneumonia is as an acute respiratory illness. • Associated with recently developed radiological pulmonary shadowing that may be segmental, lobar or multilobar. • Pneumonia is categorized in 1 of 4 ways: • 1) Community-acquired (CAP) • 2) Health care-associated (HCAP) • 3) Hospital-acquired (HAP) • 4) Ventilator-associated (YAP) • HCAP is defined to exclude HAP and YAP

Pneumonia Risk factors
 each year.")
1 - Community-acquired pneumonia • Estimated 5– 11/1000 adults suffer from (CAP) each year. • CAP may affect all age groups but is common at the extremes of age; worldwide, CAP continues to kill more children than any other illness. • Most cases are spread by droplet infection • Streptococcus pneumoniae remains the most common infecting agent. • Viral infections are recognized as important causes of CAP in children and their contribution to adult CAP is increasingly recognized. • Most cases of CAP result from aspiration of oropharyngeal secretions because the majority of organisms that cause CAP are normal inhabitants of the pharynx. • CAP can be organized into 2 groups based on the organisms that cause disease. (Typical , Atypical)
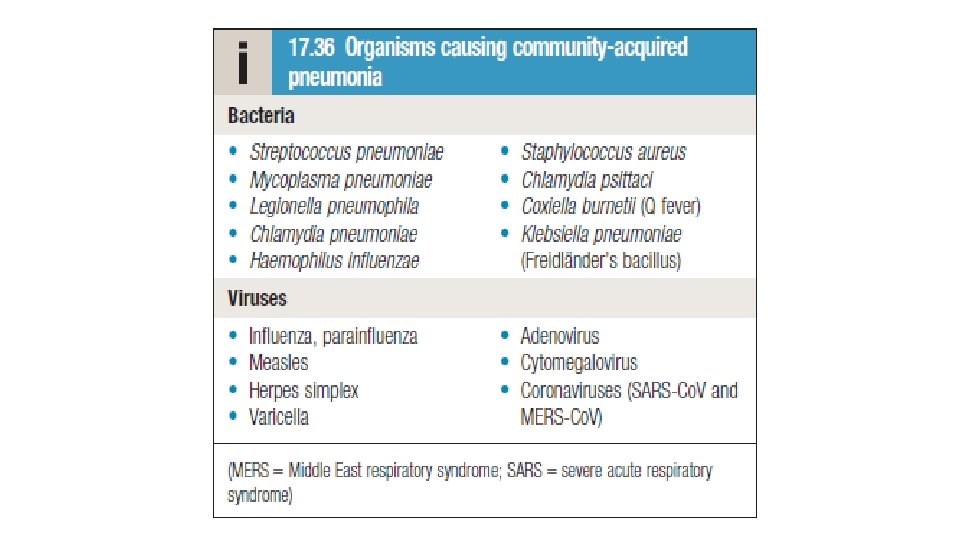
 Typical CAP a. S. pneumoniae (60%) b. Haemophilus influenzae (15%) c. Aerobic gram-negative")
1) Typical CAP a. S. pneumoniae (60%) b. Haemophilus influenzae (15%) c. Aerobic gram-negative rods (6% to 10%)—Klebsiella (and other Enterobacteriaceae) d. S. aureus (2% to 10%) 2) Atypical CAP a. Mycoplasma pneumoniae (most common) b. Chlamydia pneumonia c. Chlamydia psittaci d. Coxiella burnetii (Q fever) e. Legionella spp. f. Viruses: influenza virus (A and B), adenoviruses, parainfluenza virus, RSV 2. “Atypical” pneumonia refers to organisms not visible on Gram stain and not culturable on standard blood agar. (require special media), and they are resistant to B-lactam antibiotics. We rarely determine which bug is causing a patient's community-acquired pneumonia, but there are some risk factors associated with certain pathogens.

Typical CAP Clinical features Symptoms • • Acute onset of fever and shaking chills Dyspnea Cough productive of thick, purulent sputum Pleuritic chest pain (suggests pleural effusion) • Signs • Tachycardia, tachypnea • Late inspiratory crackles, bronchial breath sounds, increased tactile and vocal fremitus, dullness on percussion • Pleural friction rub (associated with pleural effusion) Chest radiograph (CXR) • a. Lobar consolidation • b. Multilobar consolidation indicates very serious illness

Atypical CAP Clinical features Symptoms • Insidious onset—headache, sore throat, fatigue, myalgias • Dry cough (no sputum production) • Fevers (chills are uncommon) Signs • Pulse-temperature dissociation—normal pulse in the setting of high • Wheezing, rhonchi, crackles CXR • Diffuse reticulonodular infiltrates • Absent or minimal consolidation

Clinical features General • Nausea, vomiting, and diarrhea. Elderly patients are also often confused. • Cough, which at first is short, painful and dry, but later is accompanied by mucopurulent sputum. Rust-coloured sputum may be produced by patients with Strep. Pneumoniae infection • Patient may report haemoptysis • Upper abdominal tenderness sometimes in patients with lower lobe pneumonia or those with associated hepatitis. Less typical presentations may be seen in the very young and the elderly.

Clinical features It may be possible to infer the likely agent from the clinical context. • Mycoplasma pneumoniae is more common in young people and rare in the elderly. • Haemophilus influenzae is more common in the elderly, particularly if underlying lung disease is present. • Staph. aureus is more common following an episode of influenza. • Legionella pneumophila occurs in local outbreaks centered on contaminated cooling towers in hotels, hospitals and other industries , common in organ transplant recipients, patients with renal failure, patients with chronic lung disease, and smokers and presents with GI symptoms and hyponatremia. Legionella pneumoniais rare in healthy children and young adults. • HIV-positive patients are at risk for P. carinii and M. tuberculosis, but are still more likely to have a typical infectious agent. • In nursing home residents, consider a nosocomial pathogen and predilection for the upper lobes (e. g. , Pseudomonas). • Klebsiella pneumonia has a specific association with alcohol abuse and often presents with a particularly severe bacteremia illness. • Recent foreign travel raises the possibility of infections that may otherwise be unusual e. g. MERScoronavirus • Certain occupations may be associated with exposure to specific bacteria.

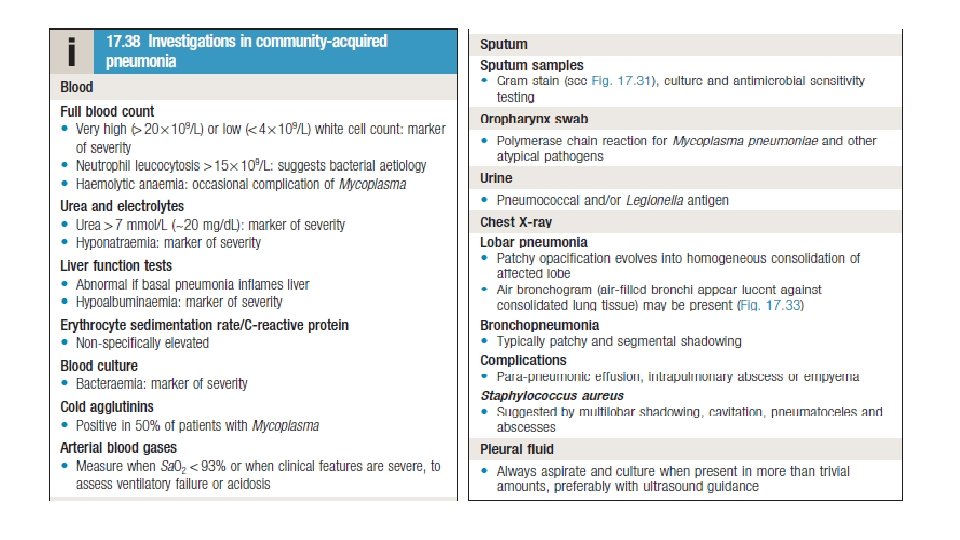
Diagnosis 1 - PA and lateral CXR required to confirm the diagnosis • a. Considered sensitive—if CXR findings are not suggestive of pneumonia, do not treat the patient with antibiotics. • b. After treatment, changes evident on CXR usually lag behind the clinical response (up to 6 weeks). • c. Changes include interstitial infiltrates, lobar consolidation, and/or cavitation. • d. False-negative chest radiographs occur with neutropenia, dehydration, infection with PCP (Pneumocystis carinii pneumonia), and early disease (<24 hours). CXR is the only reasonable method of differentiating between pneumonia and acute bronchitis.

Diagnosis 2 -Sputum • a. Sputum Gram stain — try to obtain in all patients. Commonly contaminated with oral secretions. • b. Sputum culture—try to obtain in all patients requiring hospitalization. 3 - Special stains of the sputum in selected cases. • a. Acid-fast stain (Mycobacterium spp. ) if tuberculosis (TB) is suspected. • b. Silver stain (fungi, P. carinii) for HIV/immunocompromised patients. 4 - Urinary antigen assay for Legionella in selected patients. • a. This test is very sensitive. • b. The antigen persists in the urine for weeks (even after treatment has been started). 5 - Consider two pretreatment blood cultures from different sites. Blood cultures positive in 5% to 15% of cases.

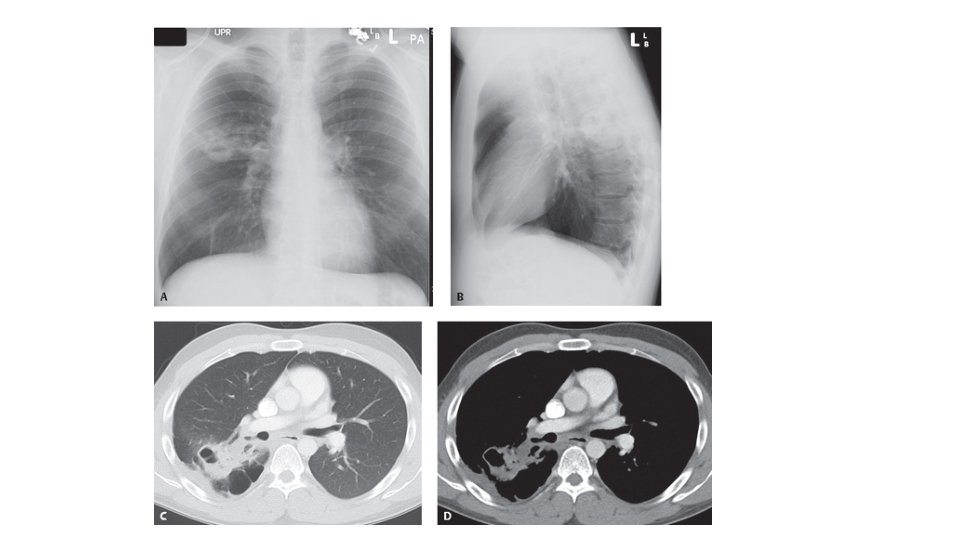
Radiograph • ‘Lobar pneumonia’ is a radiological and pathological term referring to homogeneous consolidation of one or more lung lobes, often with associated pleural inflammation; • ‘ bronchopneumonia ’ refers to more patchy alveolar consolidation associated with bronchial and bronchiolar inflammation, often affecting both lower lobes.

Right upper lobe Pneumonia

bronchopneumonia

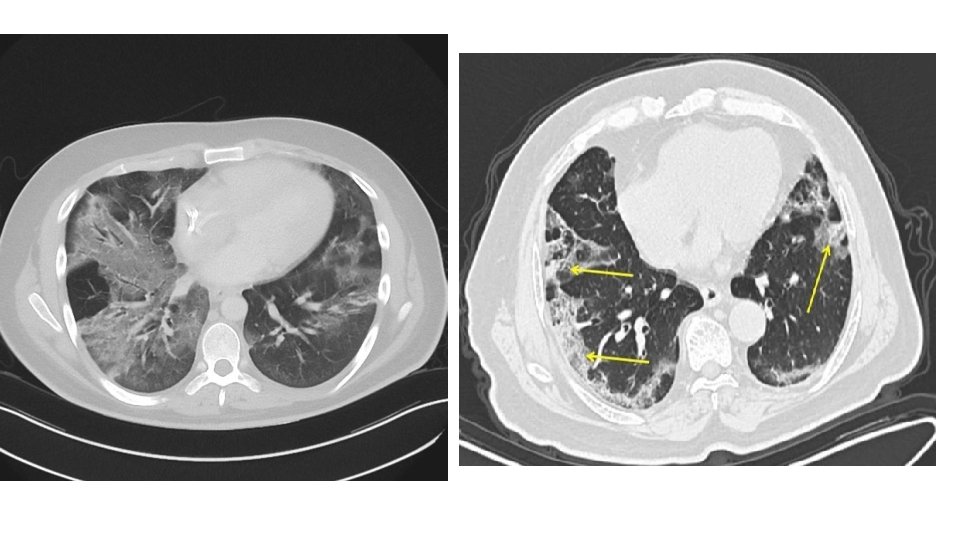
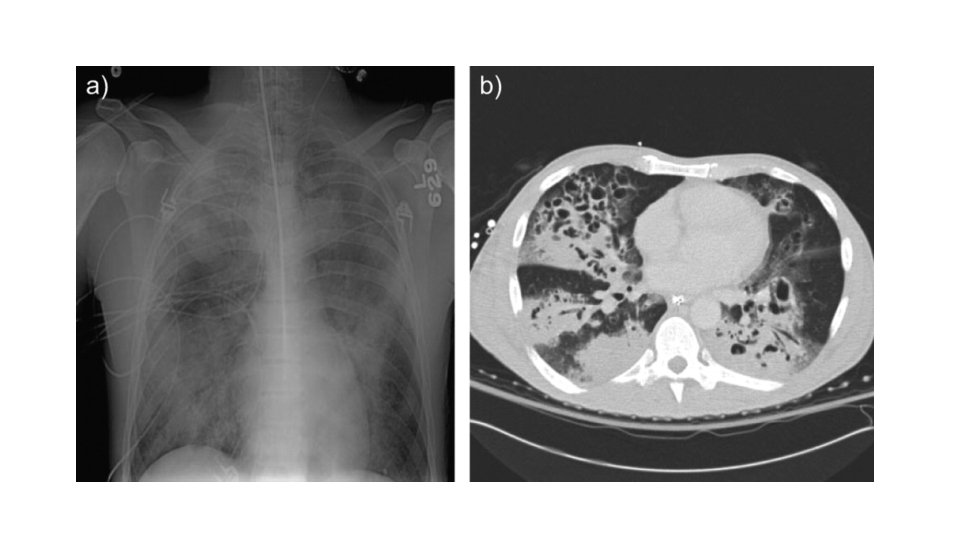
Pneumonia CT scan

Blood cultures should be done on patients with: • sepsis, • severe or unresponsive CAP, • COPD • liver disease, • history of alcohol abuse • cavitary infiltrates • asplenia • pleural effusion • leukopenia, • and/oral positive pneumococcal urine antigen test. do not do blood cultures in admitted patients who don't meet these indications or on outpatients with CAP. Do a sputum Gram stain and culture in patients with: • severe or unresponsive CAP, • COPD, • pleural effusion. • history of alcohol abuse, • cavitary infiltrates

Management
 Determine Inpatient versus Outpatient • Recommendation. In addition to clinical judgement we")
Management 1) Determine Inpatient versus Outpatient • Recommendation. In addition to clinical judgement we use a validated clinical prediction rule for prognosis, the Pneumonia Severity Index (PSI) over the CURB-65 Recommendation based on clinical judgement too Pneumonia Severity Index PSI
 Inpatient General Medical versus Higher Levels of Inpatient Treatment Intensity • Direct admission")
2) Inpatient General Medical versus Higher Levels of Inpatient Treatment Intensity • Direct admission to an ICU for patients with hypotension requiring vasopressors or respiratory failure requiring mechanical ventilation • patients not requiring vasopressors or mechanical ventilator support, we suggest using the IDSA/ATS 2007 minor severity criteria together with clinical judgment to guide the need for higher levels of treatment intensity
 and the American Thoracic Society (ATS)")
The Infectious Disease Society of America (IDSA) and the American Thoracic Society (ATS)
 • In inpatient adults with nonsevere CAP")
Empiric Treatment of CAP in Adults (Inpatient) • In inpatient adults with nonsevere CAP without risk factors for MRSA or P. aeruginosa we recommend the following empiric treatment regimens: • Combination therapy with a b-lactam and a macrolide (or doxycycline) • • Ampicillin/sulbactam cefotaxime ceftriaxone ceftaroline + • azithromycin • clarithromycin • doxycycline (for adults with CAP who have contraindications to both macrolides and fluoroquinolones) • Or • Monotherapy with a respiratory fluoroquinolone (levofloxacin, moxifloxacin )
 In inpatient adults with severe CAP without")
Empiric Treatment of CAP in Adults (Inpatient) In inpatient adults with severe CAP without risk factors for MRSA or P. aeruginosa, we recommend: • a b-lactam plus a macrolide • Or • a b-lactam plus a respiratory fluoroquinolone
")
Empiric Treatment of CAP in Adults (Inpatient)
 For outpatient adults with comorbidities such as")
Empiric Treatment of CAP in Adults (Outpatient) For outpatient adults with comorbidities such as chronic heart, lung, liver, or renal disease; diabetes mellitus; alcoholism; malignancy; or asplenia we recommend: • Combination therapy: • • • amoxicillin/clavulanate or cefpodoxime or cefuroxime + • • • azithromycin clarithromycin Doxycycline • OR Monotherapy: respiratory fluoroquinolone (levofloxacin moxifloxacin or gemifloxacin)
 • For Healthy outpatient adults without comorbidities")
Empiric Treatment of CAP in Adults (Outpatient) • For Healthy outpatient adults without comorbidities (chronic heart, lung, liver, or renal disease; diabetes mellitus; alcoholism; malignancy; or asplenia ) or risk factors for antibiotic resistant pathogens, • amoxicillin or doxycycline or a macrolide (azithromycin or clarithromycin) only in areas with pneumococcal resistance to macrolides <25% • Antibiotic therapy should be continued until the patient achieves stability and for no less than a total of 5 days • Failure to achieve clinical stability within 5 days is associated with higher mortality and worse clinical outcomes. Such failure should prompt assessment for a pathogen resistant to the current therapy and/or complications of pneumonia (e. g. , empyema or lung abscess) or for an alternative source of infection and/or inflammatory response

Use of Corticosteroids, Antiinfluenza treatment Corticosteroids • Recommendations are on the use of corticosteroids in patients with CAP and refractory septic shock , not routinely using corticosteroids in adults with nonsevere CAP , severe CAP, severe influenza pneumonia Antiinfluenza treatment • Viral CAP (Test Positive for Influenza): 1. Recommended that antiinfluenza treatment, such as oseltamivir, be prescribed for adults with CAP who test positive for influenza in the inpatient and outpatient setting, independent of duration of illness before diagnosis 2. Recommended that standard antibacterial treatment be initially prescribed for adults with clinical and radiographic evidence of CAP who test positive for influenza in the inpatient and outpatient settings

Management • Oxygen should be administered to all patients with tachypnoea, hypoxaemia, hypotension or acidosis , Continuous positive airway pressure (CPAP) should be considered in those who remain hypoxic despite high-concentration oxygen therapy. • Fluid balance Intravenous fluids should be considered in those with severe illness, in older patients and those with vomiting. An adequate oral intake of fluid should be encouraged. • Treatment of pleural pain For the majority, simple analgesia with paracetamol, co-codamol or NSAIDs is sufficient. Physiotherapy is not usually indicated in patients with CAP, although it may be helpful to assist expectoration in patients who suppress cough because of pleural pain.

Patient monitoring • For patients with pneumonia of mild to moderate clinical severity, the time to resolution of cough, decreasing sputum production, and fever, as well as other constitutional symptoms of malaise, nausea, vomiting, and lethargy, should be noted. • If the patient requires supplemental oxygen therapy, the amount and need should be assessed regularly. • A gradual and persistent improvement in the resolution of these symptoms and therapies should be observed. Initial resolution of infection should be observed within the first 2 days of therapy and progression to complete resolution within 5 to 7 days (usually no more than 10 days). • The majority of hospitalized patients with CAP should be switched from IV to oral therapy when hemodynamically stable, improving clinically as described above, have normal gastrointestinal tract function, and be able to ingest oral medications
 or nosocomial pneumonia • It is")
2 - Hospital-acquired pneumonia • Hospital-acquired pneumonia (HAP) or nosocomial pneumonia • It is the second most common hospitalacquired infection (HAI) and the leading cause of HAI-associated death. • The elderly are particularly at risk, as are patients in intensive care units, especially when mechanically ventilated. • Most common bacterial pathogens are gram-negative rods (Escherichia coli, Pseudomonas) and Staphylococcus aureus

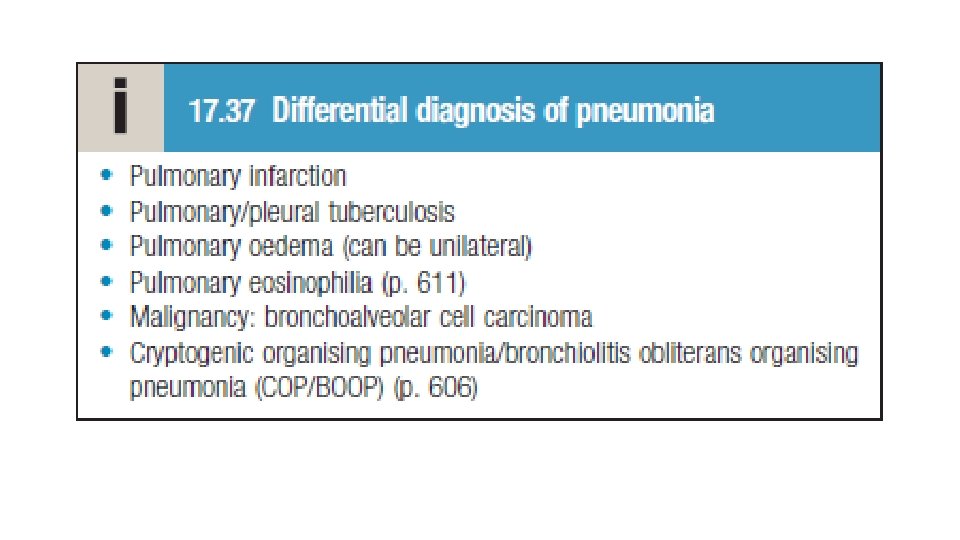
Clinical features and investigation • The diagnosis should be considered in any hospitalized or ventilated • The clinical features and radiographic signs are variable and non-specific, • Patient who develops purulent sputum (or endotracheal secretions), new radiological infiltrates, an otherwise unexplained increase in oxygen requirement, a core temperature > 38. 3°C, and a leukocytosis or leucopenia. • Differential diagnosis that includes pulmonary embolism, ARDS, pulmonary oedema, pulmonary haemorrhage and drug toxicity. • Therefore, in contrast to CAP, microbiological confirmation should be sought whenever possible. • In patients who are mechanically ventilated, bronchoscopy-directed protected brush specimens, bronchoalveolar lavage (BAL) or endotracheal aspirates may be obtained.

Management • The management is similar to CAP, focusing on oxygenation, fluid balance and antibiotics. • Treatment is tailored toward gram-negative rods (any of the following three are appropriate): a. Cephalosporins with pseudomonal coverage: ceftazidime or cefepime b. Carbapenems: imipenem c. Piperacillin/tazobactam • Macrolides are not used as single-agent therapy (as they are in CAP) • Physiotherapy is important to aid expectoration in the immobile and elderly, and adequate nutritional support is often required.

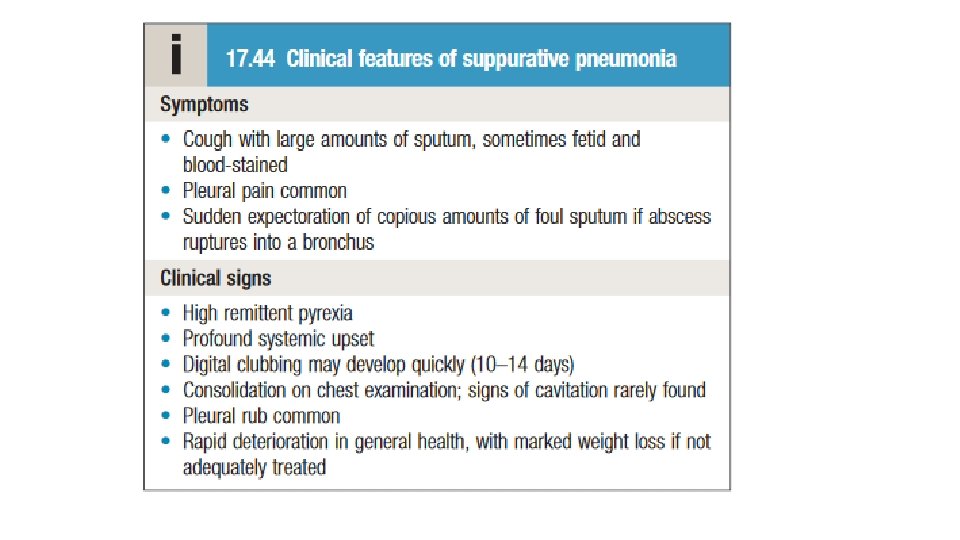
3 - Suppurative pneumonia, aspiration pneumonia and pulmonary abscess • These conditions are considered together. • Suppurative pneumonia is characterized by destruction of the lung parenchyma by the inflammatory process. microabscess formation is a characteristic histological feature. • ‘pulmonary abscess’ is usually taken to refer to lesions in which there is a large localized collection of pus, or a cavity lined by chronic inflammatory tissue, from which pus has escaped by rupture into a bronchus. • Suppurative pneumonia and pulmonary abscess often develop after the inhalation of septic material during operations on the nose, mouth or throat, under general anaesthesia, or of vomitus during anaesthesia or coma, particularly if oral hygiene is poor. • Additional risk factors for aspiration pneumonia include bulbar or vocal cord palsy, achalasia or oesophageal reflux, and alcoholism. • Aspiration tends to localize to dependent areas of the lung, such as the apical segment of the lower lobe in a supine patient.

Suppurative pneumonia, aspiration pneumonia and pulmonary abscess • Infections are usually due to a mixture of anaerobes and aerobes in common with the typical flora encountered in the mouth and upper respiratory tract. • When suppurative pneumonia or a pulmonary abscess occurs in a previously healthy lung, the most likely infecting organisms are Staph. aureus or K. pneumoniae. • Bacterial infection of a pulmonary infarct or a collapsed lobe may also produce a suppurative pneumonia or lung abscess. The organism(s) isolated from the sputum include Strep. pneumoniae, Staph. aureus, Streptococcus pyogenes, H. influenzae and, in some cases, anaerobic bacteria. In many cases, however, no pathogen can be isolated, particularly when antibiotics have been given

Investigations • Radiological features of suppurative pneumonia include homogeneous lobar or segmental opacity consistent with consolidation or collapse. • Abscesses are characterized by cavitation and a fluid level. Occasionally, a pre-existing emphysematous bulla becomes infected and appears as a cavity containing an air–fluid level.

Management • Aspiration pneumonia can usually be treated with amoxicillin and metronidazole. • Prolonged treatment for 4– 6 weeks may be required in some patients with lung abscess. • Established pulmonary actinomycosis requires 6– 12 months’ treatment with intravenous or oral penicillin, or with a tetracycline in penicillin-allergic patients. • Physiotherapy is of great value • In most patients there is a good response to treatment, and although residual fibrosis and bronchiectasis are common sequelae, these seldom give rise to serious morbidity. • Surgery should be contemplated if no improvement occurs despite optimal medical therapy. Removal or treatment of any obstructing endobronchial lesion is essential.

4 - Pneumonia in the immunocompromised patient • Patients immunocompromised by drugs or disease (particularly human immunodeficiency virus (HIV) infection are at increased risk of pulmonary infection and pneumonia is the most common cause of death in this group. • The majority of infections are caused by the same pathogens that cause pneumonia in immunocompetent individuals, but in patients with more profound immunosuppression less common organisms may become ‘opportunistic’ pathogens. • Depending on the clinical context, clinicians should consider the possibility of Gram-negative bacteria, especially P. aeruginosa, viruses, fungi, mycobacteria, and less common organisms such as Nocardia spp. Infection is often due to more than one organism.

Clinical features • Fever, cough and breathlessness but are influenced by the degree of immunosuppression, and the presentation may be less specific in the more profoundly immunosuppressed. Infections Investigations : • focal unilateral airspace opacification favours bacterial infection • bilateral opacification • cavitation may be seen • the presence of a ‘halo sign’ (a zone of intermediate attenuation between the nodule and the lung parenchyma) may suggest aspergillosis • pleural effusions suggest pyogenic bacterial infections

Management • Factors that favor a bacterial aetiology include neutropenia, rapid onset and deterioration. In these circumstances, broad-spectrum antibiotic therapy should be commenced immediately, e. g. a thirdgeneration cephalosporin, or a quinolone, plus an antistaphylococcal antibiotic, or an antipseudomonal penicillin plus an aminoglycoside. • Thereafter, treatment may be tailored according to the results of investigations and the clinical response. Depending on the clinical context and response to treatment, antifungal or antiviral therapies may be added.

Prevention • Current smokers should be advised to stop. • a. Influenza vaccine—give yearly to people at increased risk for complications and to healthcare workers • b. Pneumococcal vaccine—for patients >65 years and for younger people at high risk (e. g. , those with heart disease, cochlear implants, sickle cell disease, pulmonary disease, diabetes, alcoholic cirrhosis, asplenia) • In resource-poor settings, tackling malnourishment and indoor air pollution, and encouraging immunization against measles, pertussis and Haemophilus influenzae type b are particularly important in children. • To minimize the risk of developing VAP, healthcare providers should seek to minimize colonization of the aerodigestive tract, prevent aspiration (head raised 45 degrees), and limit the length of mechanical ventilation
—Can be seen in more than 50% of patients")
Complications • Pleural effusion (“parapneumonic effusions”)—Can be seen in more than 50% of patients with CAP on routine CXR. Empyema is infrequent in these patients. • b. Most of these effusions have an uncomplicated course and resolve with treatment of the pneumonia with antibiotics. • c. Thoracentesis should be performed if the effusion is significant (>1 cm on lateral decubitus film).

Thank you Davidson's Principles and Practice of Medicine 23 rd Edition Medstudy Internal Medicine core 16 th Edition Step-up to Medicine 5 th Edition Therapeutics Lower Respiratory Tract infection
- Slides: 48