Autocrine Paracrine Pharmacology Part 11 Prof AZZA ELMEDANY
 Prof. AZZA EL-MEDANY")






 Diamine oxidase Methyl imidazole acetic acid")






 Has a Sedating effect Clinical uses : Insomnia Motion sickness")
 Non-sedating effect Clinical uses Allergic conditions as : allergic rhinitis Conjunctivitis")









 ( bronchorelaxation )")





")
 Abortion Induce abortion in first trimester.")
 Treatment of postpartum haemorrhage ( vasoconstriction + uterine muscle contraction)")



- Slides: 38
Autocrine & Paracrine Pharmacology (Part 11) Prof. AZZA EL-MEDANY
OBJECTIVES At the end of lecture the Students should be able to: 1 - Specify storage sites of histamine 2 - Explain the synthesis, release & inactivation of histamine 3 -List histamine receptors regarding: Type, major location, major biologic effects 4 -Explain the clinical uses of histamine receptors antagonists.
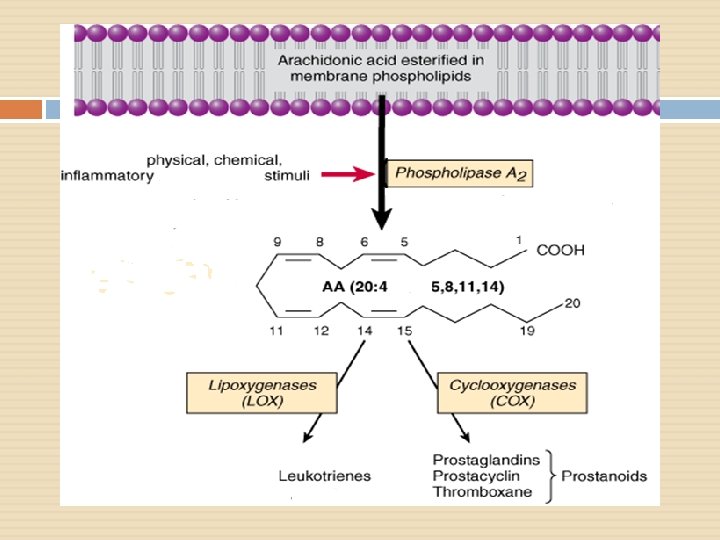
Continue 5 - Describe the synthesis of eicosanoids 6 - Classify drugs that inhibit synthesis of eicosanoids 7 - Enumerate the pharmacological actions of eicosanoids 8 -Enumerate the clinical uses of PGs analogs
CLASSIFICATION OF MEDIATORS EICOSANOIDS PEPTIDES Prostanoids Contractants Angiotensin Endothelin Prostaglandins Thromboxane A 2 NO Leukotrienes Vasopressin …. etc. Tachykinins [SP] Histamine Serotonin …etc ATP / ADP Adenosine Chemokine Growth Factors Relaxants Kinines PURINES Cytokines NPY ANP MONOAMINES OTHERS VIP
H istamine Neurotransmitte r Allergic & Inflammatory reactions Gastric acid secretion
Storage Sites Highest amounts in mast cells Basophils Skin Lung Intestinal mucosa Stomach Brain
Biosynthesis
Inactivation Histamine Imidazole N-methyltransferase Methyl histamine (Oxidation) Diamine oxidase Methyl imidazole acetic acid
H 1 H 2 H H 3 -ve presynaptic 3 + + + H 1
RELEASE v. Primary mechanism during allergic reactions [ Ig. E antibody interacts with antigen on the surface of mast cells ]
Continue v v Enzymes as trypsin or drugs as morphine or other chemicals can liberate histamine Tissue injury by trauma or burn
Histamine receptors Receptor Type Major Tissue Locations Major Biologic Effects H 1 smooth muscle, endothelial cells acute allergic responses H 2 gastric parietal cells secretion of gastric acid H 3 central nervous system neurotransmission H 4 mast cells, eosinophils, T cells regulating immune responses
Adverse Effects Of Histamine Hypotension, tachycardia, flushing Headache, visual disturbances, increase skin temperature Bronchoconstriction, dyspnea, diarrhea
Histamine receptors antagonists
Diphenhydrami n (First generation) Has a Sedating effect Clinical uses : Insomnia Motion sickness Allergic conditions H 1 antagonists ( Blockers )
Loratadine (Second generation) Non-sedating effect Clinical uses Allergic conditions as : allergic rhinitis Conjunctivitis Urticaria H 1 antagonists
Cimetidine H 2 antagonists Inhibitor of gastric acid secretion Used in the treatment of peptic ulcers
BETAHISTINE H 3 antagonists Used in treatment of vertigo in middle ear
EICOSANOI DS
INHIBITORS OF EICOSANOIDS
Drugs Phospholipids Corticosteroids Zileuton Lipoxygenase Phospholipase A 2 Arachidonic Acid NSAIDs Cyclooxygenase Leukotrienes Prostaglandins Prostacyclin Thromboxane (TXA 2)
Comparison in actions between Prostaglandins Thromboxane A 2
Vascular smooth muscles: Prostaglandins Potent vasodilators. Thromboxane A 2 Potent vasoconstrictor.
Blood: TXA 2 a potent inducer of platelet aggregatio n. Prostaglandins inhibit platelet aggregation
Inflammation: Both play important role in Ø inflammatory reactions.
Bronchial smooth muscle: -Prostaglandins -Thromboxane (bronchoconstriction) ( bronchorelaxation )
Uterine smooth muscle: Prostaglandins increase uterine contractions → Menstruation/ Dysmenorrhea/ Labor contractions
GIT smooth muscle: - Prostaglandins IT G motility
GIT secretions: Prostaglandins ↓acid secretion Mucin secretion
Kideny Prostaglandins increase renal blood flow and diuresis.
Central and peripheral nervous systems Fever
Clinical uses of prostaglandins analogs ( Synthetic prostaglandins )
Carboprost 1) Abortion Induce abortion in first trimester.
2) Treatment of postpartum haemorrhage ( vasoconstriction + uterine muscle contraction)
Latanoprost eye drops /in treatment of open angle glaucoma. (↓ IOP by enhancing outflow of the aqueous humar)
Misoprostol Treatment of Peptic ulcer
Thank you