Theory Evaluation of Penders Health Promotion Model HPM
 Nursing 8440 November 26,")














 by Pender and colleagues")





 • Research methodology reflects")

 • Special education and skill training")


- Slides: 27
Theory Evaluation of Pender’s Health Promotion Model ( HPM ) Nursing 8440 November 26, 2012 Jennifer Bauman, RN, BA, PCCN
Purpose and Topics • • • Critically evaluate Nola J. Pender’s Health Promotion Model (HPM) High prevalence and cost of conditions that are caused by poor lifestyle choices – conditions that are largely preventable According to Pender (1996), “in the United States, it is estimated that unhealthy lifestyles are responsible for 54% of the years of life lost prior to age 65, environment for 22%, and heredity for 16%” ( p. 5). Potential to decrease the pervasiveness of lifestyle-related conditions and achieving cost savings through health promotion and illness prevention. Topics – Background of author and overview of theory – Historical development of theory – Origins – Main structural elements – Ongoing development of theory – Critique of theory using Fawcett’s theory evaluation recommendations
Nola J. Pender: Background • Born 1941 in Lansing, Michigan • Masters degree in human growth and development at Michigan State University in 1965 • “’The M. A. in growth and development influenced my interest in health over the human lifespan. This background contributed to the formation of a research program for children and adolescents, ’ stated Pender” (Sakraida, 2006, p. 453). • Ph. D in psychology and education in 1969 at Northwestern University in Evanston, Illinois • Dissertation in 1970 investigated developmental changes in encoding processes of short-term memory in children • “Pender credits Dr. James Hall, a doctoral program advisor, with ‘introducing me to considerations of how people think and how a person’s thoughts motivate behavior’” (Sakraida, 2006, p. 453). • Shift in her thinking toward defining the goal of nursing care as the optimal health of the individual • Influenced by Dr. Beverly Mc. Elmurry at Northern Illinois University and the book, High. Level Wellness, by Halpert Dunn (1961) • Also influenced by husband Albert Pender, associate professor of business and economics
Overview “The HPM is an attempt to depict the multidimensional nature of persons interacting with their environment as they pursue health” (Pender, 1996, p. 53).
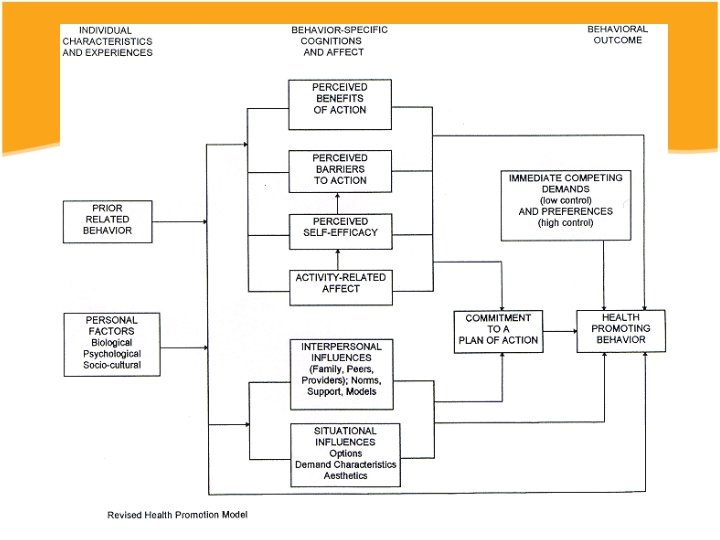
Overview • Behaviors motivated by prior related health promotion behaviors and personal factors – Biological, psychological, sociocultural • Weighs benefits and barriers of health promoting actions – Perceived self-efficacy – Affect related to the specific activity – Interpersonal and situational influences • Commit to a plan of action to promote health – Immediate competing demands • Adopts the health promoting behavior. • Client plays an ACTIVE role in initiating and maintaining health promotion behaviors, as well as altering the environment to be successful
HPM
Historical Development of Theory • 1975 first published in Nursing Outlook, « A Conceptual Model for Preventative Health Behavior » • 1982 HPM first in nursing literature • 1987 HPM in Health Promotion in Nursing Practice • 1996 revised HPM after six year study
Origins • Philosophical origins: “Reciprocal Interaction World View, in which humans are viewed holistically, but parts can be studied in the context of the whole. Human beings interact with their environment and shape it to meet their needs and goals” (Pender, 2011, p. 2). • Theoretical origins: derived inductively from many psychological theories, especially expectancy-value theory and social cognitive theory
Expectancy-Value Theory of Human Motivation • Initially conceptualized by Norman T. Feather in 1982 • States that “individuals engage in actions to achieve goals that are perceived as possible and that result in valued outcomes” (Pender, 2011, p. 2). • Emphasizes that human behavior is rational and economical (Syx, 2008).
Social Cognitive Theory • Originally published by Albert Bandura in 1977 • “…Thoughts, behavior, and environment interact. For people to alter how they behave, they must alter how they think” (Pender, 2011, p. 2). • Self-efficacy, which is “a judgment of one’s ability to carry out a particular course of action” (Pender, 1996, p. 54) • Greater perceived self-efficacy results in persistent engagement in behavior despite obstacles.
Main Structural Elements: Assumptions • • Reflect the behavioral science perspective and emphasize the active role of the patient for managing health behaviors through environmental modification (Sakraida, 2006) Seven Assumptions: – 1. “Persons seek to create condition of living through which they can express their unique human health potential. ” – 2. “Persons have the capacity for reflective self-awareness, including assessment of their own competencies. ” – 3. “Persons value growth in directions viewed as positive and attempt to achieve a personally acceptable balance between change and stability. ” – 4. “Individuals seek to actively regulate their own behavior. ” – 5. “Individuals in all their biopsychosocial complexity interact with the environment, progressively transforming the environment and being transformed over time. ” – 6. “Health professionals constitute a part of the interpersonal environment, which exerts influence on persons throughout their lifespans. ” – 7. “Self-initiated reconfiguration of person-environment interactive patterns is essential to behavioral change. ”
Main Structural Elements: Concepts • Three categories: – Individual characteristics and experiences • Prior related behavior and personal factors • Importance of their effects depends on target behavior and population – Behavioral-specific cognitions and affect • Major motivational significance and modifiable through nursing actions • Perceived benefits of action, perceived barriers to action, perceived self-efficacy, activity-related affect, interpersonal influences, and situational influences – Behavioral outcomes • Commitment to a plan of action, immediate competing demands and preferences, and health-promoting behavior (the end-point or action outcome in HPM)
Main Structural Elements: Theoretical Assertions The assertions emphasize that the HPM contains a competence- or approach-oriented focus, unlike other health behavior theories which are avoidance-oriented models that rely upon fear or threat to health as motivation for health behavior. In Pender’s theory, health promotion is motivated by the desire to increase well-being and actualize human potential (Sakraida, 2006).
1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. Prior behavior and inherited and acquired characteristics influence beliefs, affect, and enactment of health-promoting behavior. Persons commit to engaging in behaviors from which they anticipate deriving personally valued benefits. Perceived barriers can constrain commitment to action, mediator of behavior, and actual behavior. Perceived competence or self-efficacy to execute a given behavior increases the likelihood of commitment to action and actual performance of behavior. Greater perceived self-efficacy results in fewer perceived barriers to specific health behavior. Positive affect toward a behavior results in greater perceived self-efficacy, which can, in turn, result in increased positive affect. When positive emotions or affect are associated with a behavior, the probability of commitment and action are increased. Persons are more likely to commit to and engage in health-promoting behaviors when significant others model the behavior, expect the behavior to occur, and provide assistance and support to enable the behavior. Families, peers, and health care providers are important sources of interpersonal influence that can increase or decrease commitment to and engagement in health-promoting behavior. Situational influences in the external environment can increase or decrease commitment to or participation in health-promoting behavior. The greater the commitment to a specific plan of action, the more likely health-promoting behaviors are to be maintained over time. Commitment to a plan of action is less likely to result in the desired behavior when competing demands over which persons have little control require immediate attention. Commitment to a plan of action is less likely to result in the desired behavior when other actions are more attractive and thus preferred over the target behavior. Persons can modify cognitions, affect, and the interpersonal and physical environments to create incentive for health actions.
Ongoing Development • Revision from 1987 to 1996 • “The 1996 revisions intended to increase utility of the model for prediction and intervention in health behaviors” (Young, Taylor, M-R, 2001, p. 308). • King (1994) critiqued Pender’s original model, stating: – Pender viewed environment, situational and interpersonal factors as modifiers of the central cognitive—perceptual factors. Pender viewed the environment as it relates to behavior rather than how it relates to health (…) Pender gave little recognition to the impact that the sociopolitical context has on the individual. Rather, Pender focused on individuals, their perception of control, their definition of health, and their decision-making capacity. (…) Pender's model is further limited as the existence or complexity of interrelationships among the factors is not acknowledged. (…) The model also does not specifically address motivating factors. (p. 214)
Pender and colleagues • Six-year, federally funded study (really, studies) by Pender and colleagues • Tested the validity of the HPM and the Health. Promoting Lifestyle Profile tool in the populations of working adults, older community-dwelling adults, ambulatory patients with cancer, and patients undergoing cardiac rehabilitation. • Proved validity and reliability of the model and tool but that revisions needed
Empirical Evidence • Studies from 1987 through 1996 investigated 5 -12 of the HPM variables, or concepts, at one time – Variance in health promoting lifestyle and behaviors explained by these concepts ranged from 19% to 59% (Pender, 1996) • Empirical findings were consistent with social learning theory (Pender, 1996) • Perceived self-efficacy, benefits, and barriers were empirically supported as predictors of health behaviors (Pender, 1996)
COGNITIVE-PERCEPTUAL FACTORS Importance of health MODIFYING FACTORS PARTICIPATION IN HEALTHPROMOTING BEHAVIOR Demographic characteristics Perceived control of health Perceived self-efficacy Definition of health Perceived health status Perceived benefits of healthpromoting behavior Perceived barriers to healthpromoting behaviors Biologic characteristics Interpersonal influences Likelihood of engaging in health-promoting behavior Situational factors Cues to action Behavioral factors
Changes from 1987 to 1996 • Deletion of “importance of health, ” “perceived control of health, ” and “cues for action” as predictors • Repositioned “definition of health, ” “perceived health status, ” and demographic and biological characteristics in the model – Included in the category of personal factors. • Added 3 variables that serve to influence the individual to engage in health-promoting behaviors: activity-related affect, commitment to a plan of action, and immediate competing demands and preferences • Overall – Direct and indirect effects of all concepts on health promoting behaviors – Each concept’s dynamic influence on the other concepts (and vice versa) – Application of certain aspects of each concept to specific health behaviors and populations, as well as to general health-promoting lifestyles.
Critique: Fawcett’s theory evaluation • Significance – Concepts, propositions, philosophical claims, and conceptual model from which theory was derived are all explicitly stated. – Authors of antecedent knowledge – expectancyvalue and social cognitive theories – are acknowledged. – Bibliographical citations are provided.
Critique, continued … • Internal consistency – Content and context of the HPM are congruent, clear, and consistent – Theory propositions reflect structural consistency • Parsimony (met when “statements clarify rather than obscure the topic of interest”) – Stated and explained clearly and concisely – However, theoretical assertions are lengthy
Testability (Theoretical concepts should be observable and the propositions measurable) • Research methodology reflects the HPM • Facilitates generation of testable hypotheses • Theory concepts are observable through appropriate, empirically proven, instruments – Health Promoting Lifestyle Profile (HPLP), which was created in 1987, tested, and revised in 1996 (HPLP II) • Data analysis techniques – Analysis of variance and hierarchical multiple regression are not appropriate due to the interactive effects of the concepts – A structural equation model should be used (Johnson et al)
Empirical Adequacy (Are the middle range theory’s assertions harmonious with the research studies’ empirical results? ) • Tested the validity of the HPM or used the HPM as a framework, in a variety of populations and with a diverse health behaviors: – Hearing protection among farmers (Mc. Cullagh, Lusk, Ronnis, 2002) – Hearing protection among construction workers (Lusk et al. , 1999, which was used to develop an interactive, video-based program to increase hearing protection use) – Hearing protection among Mexican-American workers (Kerr, Lusk, & Ronin, 2002) – Caregiver burden and health promotion (Sisk, 2000) – Physical activity in Taiwanese youth (Wu & Pender, 2005) – Women with multiple sclerosis (Stuifbergen & Roberts, 1997) – Smoking and non-smoking college students (Martinelli, 1999) – Health promotion activity in employed Mexican American women (Duffy, Rossow, Hernandez, 1996) – Long term married couples (Padula & Sullivan, 2006) – Pregnant women over age 35 (Viau, Padula, Eddy, 2002).
Pragmatic Adequacy (Use in clinical practice and research) • Special education and skill training is not essential to apply theory in clinical practice. • The HPM applies across the lifespan and is useful in a variety of settings. • Useful in clinical practice, health policy, nursing and patient education, nursing research – Difficult to derive clinical procedures/policies due to personalization
Concluding Remarks • Simple to use and understand • Generalizable to many populations and many health behaviors • Empirically proven to be valid and reliable • Future endeavors – More intervention studies needed – Health policy
Questions?