Psych 120 General Psychology Christopher Gade Office 1030












 n Depression is a family and genetic linked disorder n Life")







. –")






- Slides: 32
Psych 120 General Psychology Christopher Gade Office: 1030 A Office hours: MW 4: 30 -5: 30 Email: gadecj@gmail. com Class MW 1: 30 -4: 30 Room 2240
Today’s class… n In the final three lecture sections of the course, we’ll be discussing three major disorder groups. – Anxiety disorders – Mood disorders – Schizophrenia
Anxiety Disorders n Anxiety disorders involve an intense experience of anxiety and a series of efforts to deal with it. n Four major categories of anxiety disorders: – Generalized Anxiety Disorder – Panic Disorder – Phobias – Obsessive Compulsive Disorder
Generalized Anxiety Disorder n Is found in 5 -6% of the population. – 11, 14, 27 n Involves a pervasive and free floating anxiety. n Affected people feel continuously tense and jittery, worried, and suffer from sleeplessness. n Antidepressant medication & relaxation training have been shown to be effective treatments.
Panic Disorder n 1 -3% of the population are diagnosed with this disorder at some time in their life. – n 02, 25 Identified through the occurrence of frequent panic attacks. – Panic attacks: minutes-long episodes of intense fear that something awful is going to happen. These attacks feature… § § heart palpitations shortness of breath choking sensations trembling n Repeated incidences lead to fear of ‘panic attack’, and thus a panic disorder and associated phobias, i. e. agoraphobia. n Antidepressants and behavior therapy are sometimes beneficial treatments. n Age and time also are associated with a decrease in panic disorder occurrence rates.
Phobias n Afflicts 11% of the population during their lifetime and 5 -6% at any time. – 6, 38, 28, 15, 30 n Fears are identified as a phobia when anxiety or irrational fear of a particular object or situation are extreme enough to interfere with everyday living. n There is evidence for a genetic link in the predisposition for developing phobias, (some life experience usually must occur to cause the phobia). n Behavioral therapy that have been shown to ameliorate phobias. – systematic desensitization and flooding n Pharmacological therapy for phobias include tranquilizers and antidepressant drugs.
n Some theories for the cause of phobias: – We might be evolutionarily ‘primed’ for fear of some and situations § Snakes versus electricity – Our fears of certain objects or situations are based on amount of safe vs. scary exposures. § Airplanes versus automobiles – people are more prone to develop phobias of objects or situations that they cannot predict or control § Shark attacks Phobias (cont)
Obsessive Compulsive Disorder n Found in 2 -3% of the population n Repetitive, irresistible acts (compulsions) performed to alleviate an ongoing anxious stream of thought (obsessions) with such persistence that they interfere with normal life activities. n Typically found in average, hard working perfectionists. n Associated with guilt as much as anxiety (trying to suppress shameful thoughts/desires: cleaning compulsion, checking compulsion). n Some evidence for genetic contribution to OCD, especially in patients that develop OCD before 18 yrs. n Most will improve with or without treatment over time. n Exposure therapy is often used: present the OCD person with a situation which facilitates the obsessions and prevent them from performing the compulsions to demonstrate that nothing catastrophic will occur. – 07
Overview n All of the different disorders listed in lecture today are all classified under the anxiety disorders category in the DSM. n Each has its own prevalence, defining characteristics, and causes/solutions. n However, when looking at these disorders, they are all considered very similar by most clinical psychologists.
Mood Disorders n Mood disorders all involve long-term problems with basic emotions. All but one of the most prevalent mood disorders are associated with a negative, unpleasant mood. n There a number of mood disorders that exist, with one being the most prevalent and well known. – – Depression Seasonal Affective Disorder Dysthymia Bipolar Disorder
Depression n 5% of population is diagnosed in a given year, 1020% in their lifetime – n 17, 24, 12, 16, 7, 2, 43, 27, 33, 26 Multiple symptoms associated with the diagnosis of this disorder – feeling little interest in anything (including food and sex) – little pleasure – little motivation to be productive all day long for an extended period of time (at least 2 weeks). n Also associated with – – – A feeling of powerlessness, guilt and worthlessness Suicidal ideation and attempts sleep abnormalities
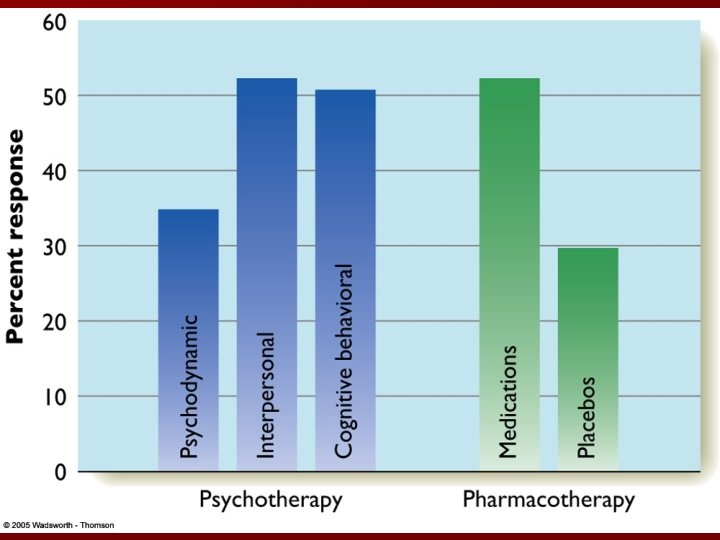
Depression (cont. ) n Depression is a family and genetic linked disorder n Life events contribute to the emergence of depression n Women are diagnosed with depression about twice as much n Cognitions are associated with depression: n Treatments for depression: n Few people remain permanently depressed – – – – – pessimistic vs. optimistic internal vs. external global vs. singular stable vs. dynamic regular sleep and exercise for mild to moderate depression ECT (no stats for major depression) placebo drug interventions psychotherapies
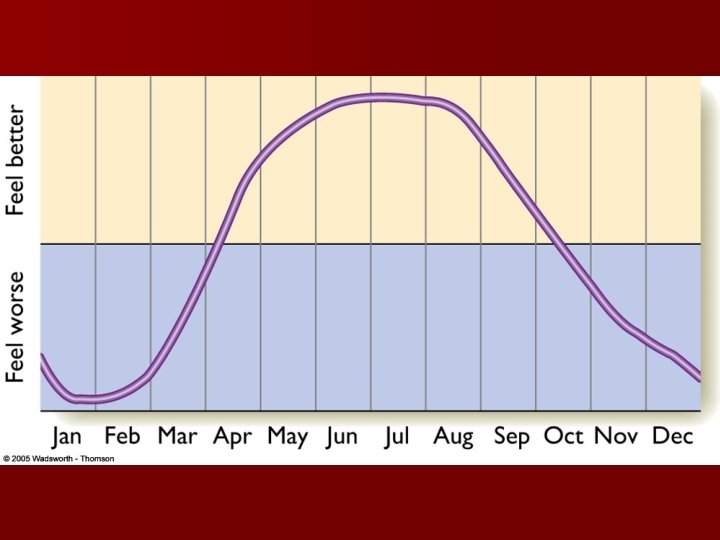
Seasonal Affective Disorder and Dysthymia n Seasonal Affective Disorder – – Associated with the change of seasons Symptoms are similar to those of depression, but to a milder extent Light therapy is a popular treatment for this disorder Prevalence of disorder depends upon location § approx 1% of Floridians § Approx 9 -10% of Minnesotans – 49, 18 n Dysthymia – – Symptoms are similar to those of depression. Much less severe symptoms Lasts much longer than depression (2 years before diagnosis) Not considered traumatic at any given time, but can be very debilitating through its long-term effects – 29, 33
Bipolar Disorder n AKA manic depressive disorder n Found in only 1% of the population n involves a person alternating between feeling depressed and feeing manic: constantly active and uninhibited, excited or irritable. n Two forms of bipolar disorder n Twin studies suggest a genetic component to Bipolar Disorder n Treatments include Lithium and anticonvulsants – 22 – Bipolar Type II (hypomania)
Overview n As in the last class, all of the different disorders listed in lecture today are all classified under the same disorders category in the DSM (affective disorders). n Each again has its own prevalence, defining characteristics, and causes/solutions. n But… again, when looking at these disorders, they are all considered very similar by most clinical psychologists.
Schizophrenia n What it is NOT: multiple personality disorder, sociopathy, or antisocial personality disorder. n What it is: a severe disconnect with reality with many cognitive and emotional symptoms. – Affects about 1% of the population § 16 – Almost identical incidence in men & women (7: 5 ratio has been found in recent studies) – Onset is usually sometime between 16 and 25 yrs old (later for women)
Diagnosis of Schizophrenia n The DSM-IV diagnosis of schizophrenia requires that the person exhibit a complete deterioration of daily activities along with at least two of the following symptoms: – – – Hallucinations Delusions or thought disorders Incoherent speech Grossly disorganized behavior Loss of normal emotional responses and social behaviors § Note: If the hallucinations or delusions are severe enough, no other symptoms are required in the diagnosis of this disorder.
More on the symptoms… n Schizophrenia symptoms are categorized into two groups – Positive Symptoms: behaviors that are present, or added to the persons repertoire of behavior as a result of the schizophrenia. – Negative Symptoms: behaviors that are diminished, or absent from the persons repertoire of behavior as a result of the schizophrenia.
Positive Symptoms n Hallucinations: perceiving things that are not there (auditory and visual). – Auditory hallucinations are much more common that visual ones. – Almost all of us occasionally have auditory (any maybe visual) hallucinations. Schizophrenics are distinguished by the frequency and complexity of these hallucinations. n Delusions: very rigid false or unfounded beliefs. – persecution: a belief that others (groups and individuals) are conspiring against or persecuting the individual (e. g. “they’re all after me”) – grandiose: a belief in unusual importance (e. g. pregnancy ‘flicks’) – reference: a tendency to interpret all messages as if they were meant for oneself (there are codes for me in the newspaper headlines) – bizarre: random delusions that don’t fall under any of the previous categories (e. g. some of my vital organs are missing)
Negative Symptoms n Flat affect: blunted expression of emotion, e. g. mask-like face, flat voice, poor eye contact. n Anhedonia: Diminished ability to experience pleasure, e. g. report little enjoyment in life, seek out few enjoyable activities. n Social Withdrawal n Inattentiveness, thought blocking (a particularly abrupt or complete interruption of thought).
Disorganized Symptoms n Disorganized speech: – – – n severe tangentiality loose associations derailment of thought Disorganized behavior: – catatonic behavior – unusual postures
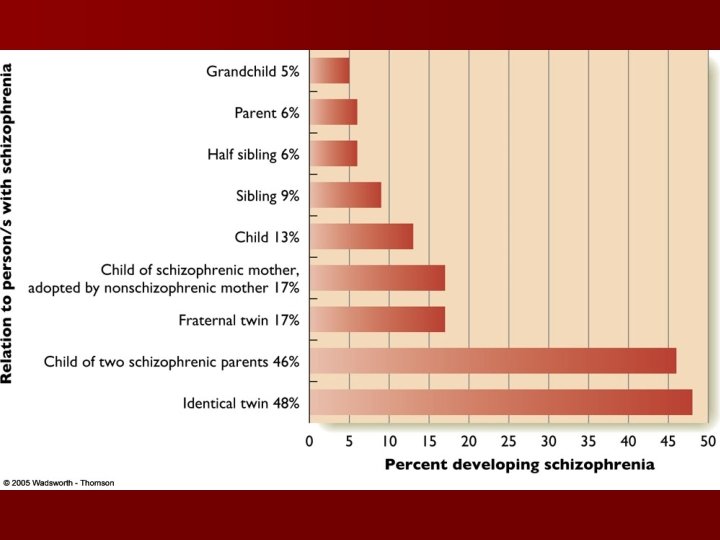
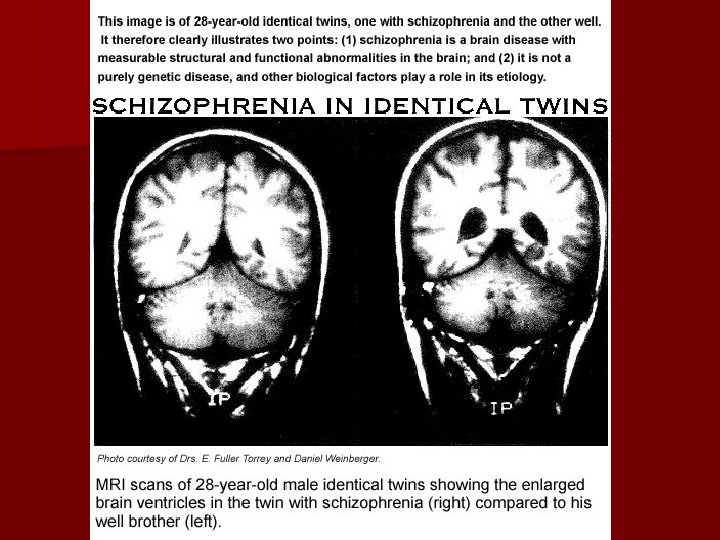
Theorized Causes n Genetic n Brain abnormality/malformation n The neurodevelopmental hypothesis – Twin studies suggest a genetic component in susceptibility for schizophrenia – No single gene has been linked to schizophrenia – the hippocampus and parts of the cerebral cortex are a little smaller than normal, the cerebral ventricles are larger than normal, the neurons are smaller there are fewer synapses in the prefrontal cortex. – Is this a causal or correlational relationship? – schizophrenia is the result of nervous system impairments that develop before and/or around the time of birth. – Caused partially though genetics, but also through environmental influences: § § § poor prenatal care difficult pregnancy and labor mother’s exposure to influenza virus.
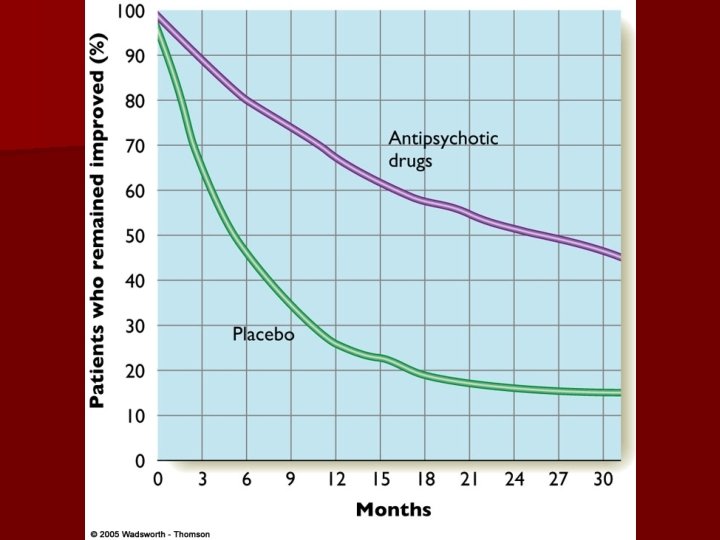
Treatments n Medication: Antipsychotic or neuroleptic drugs. n Hospitalization: useful for only acute episodes. n Cognitive Behavioral Therapy (CBT): – These all relieve symptoms for at least a little while. – Some block dopamine synapses in the brain, others effect glutamate concentration. – Most in the past produced unpleasant side effects: tardive dyskenesia. – Hallucinations: help patients perceive distinctions between internal/external – Delusions: treat self-esteem or other psychological issues – Flat affect: increase social skills – Anhedonia: increase activities.
Treatment Success n Most treatments provide temporary success almost immediately. n Over the long run, success rates wane greatly. n Success rates are highly associated with the intensity of the symptoms pre-treatment, and the time between onset and treatment of the disorder. n The Rule of thirds for medication. – Acute and sudden onset: good response to medication – Middle: could be either sudden or acute, mixed response to medication – Chronic: slow, insidious onset, poor response to medication
THE END n This marks the end of the lectures for this class. Come on time on Wednesday for the last exam. n Good luck in your studies, and thanks for spending some time with me this summer.