Pathophysiology of EndStage Renal Disease Dr Khaled Khalil





 changes in the normal portions of the kidney. These")

 Cause Percentage of Total ESRD Patients")

 ↓")


 the inability of the bladder to empty completely, leaving residual urine in the")







 water and")


- Slides: 26
Pathophysiology of End-Stage Renal Disease Dr. Khaled Khalil
By the end of this session, the student should: q. Relate the causes of chronic renal disease to renal failure. q. Describe the vicious cycle of chronic renal failure that leads to end-stage renal disease. q. Describe the changes in body homeostasis in response to loss of renal functions. Guyton & Hall Textbook of medical physiology 12 th edition. P. 401 -408
q Chronic renal failure results from progressive and irreversible loss of large numbers of functioning nephrons. q. Deterioration of the body functions related to the kidney occurs when more than 75% of nephrons are lost q. No cure is expected. Either the patient is placed on dialysis or renal transplantation is performed.
Metablolic Disorders Some Causes of Chronic Renal Failure Primary Tubular Disorders Diabetes mellitus Nephrotoxins (analgesics, heavy metals) Obesity Urinary Tract Obstruction Amyloidosis Renal calculi Hypertension Hypertrophy of prostate Renal Vascular Disorders Urethral constriction Atherosclerosis Congenital Disorders Nephrosclerosis-hypertension Polycystic disease Immunologic Disorders Glomerulonephritis Polyarteritis nodosa Lupus erythernatosus Infections Pyelonephritis Tuberculosis Congenital absence of kidney tissue (renal hypoplasia)
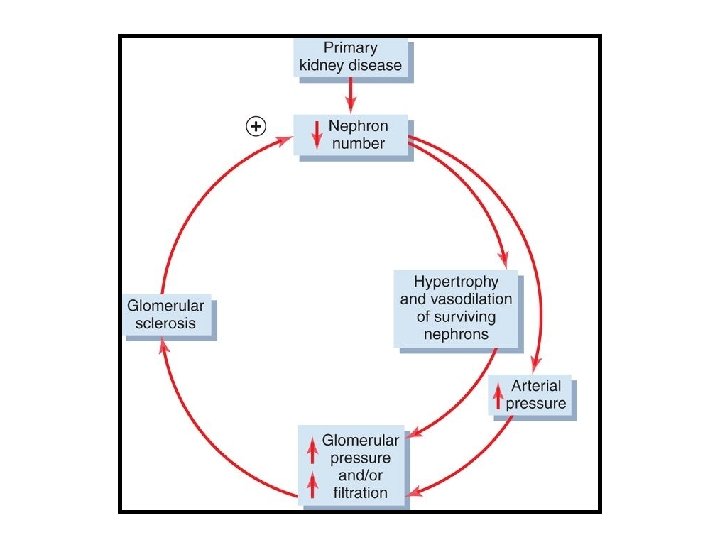
Primary renal disease Adaptive (compensatory) changes in the normal portions of the kidney. These changes include: functional changes Structural Changes Hypertrophy (growth of the various structures of the surviving nephrons). Mechanism not well understood Decrease vascular resistance and increased tubular reabsorption in the surviving nephrons q Both results in excretion of normal amounts of water and solutes even when kidney mass is reduced to 20 to 25 percent of normal. However, if primary cause continues for a prolonged periods (years) ------> adaptive changes produce more injury of the remaining nephrons -----> End-Stage Renal Disease.
What is the cause of additional injury? Not known!!!! May be due to: Compensatory V. D. of small arterioles -------> ↑ pressure and stretch of glomeruli -------> sclerosis of both arterioles and glomeruli ------> obliteration (closure) of nephrons ------> more renal loss. Evidence: Administration of ACE inhibitors or ARBs (angiotensin-receptor blockers) that decrease the hydrostatic glomerular pressure -----> slow down the renal damage. These drugs are called renoprotective drugs.
Most Common Causes of End-Stage Renal Disease (ESRD) Cause Percentage of Total ESRD Patients Diabetes mellitus 45 Hypertension 27 Glomerulonephritis 8 Polycystic kidney disease 2 Other/unknown 18 Thus, the most important risk factor for ESRD is obesity being a major cause of both diabetes and hypertension.
Injury to the Renal Vasculature Atherosclerosis of the larger renal arteries Ischemia of one kidney fibromuscular hyperplasia of one or more of the large arteries Activation of RAS Systemic hypertension Nephrosclerosis smaller interlobular arteries and in the afferent arterioles progressive thickening of the vessel wall that eventually constricts the vessels ---> occlusion Destruction of the supplied nephrons as no collaterla circulation exists
Nephroscelerosis occurs even in normal people in which renal functions (RBF & GFR) ↓ by 40 to 50 percent by age 80. The frequency and severity of nephrosclerosis and glomerulosclerosis are greatly increased by concurrent hypertension or diabetes mellitus. Benign nephrosclerosis in association with severe hypertension can lead to a rapidly progressing malignant nephrosclerosis.
Injury to the Glomeruli Acute glomerulonephritis Secondary to systemic diseases, such as lupus erythematosus Chronic glomerulonephritis Accumulation of precipitated antigen-antibody complexes in the glomerular membrane. inflammation, progressive thickening of the membranes invasion of the glomeruli by fibrous tissue Loss of glomerular functions -----> less filtration ----> renal failure
Injury to the Renal Interstitium poisons, drugs, and bacterial infections. vascular, glomerular, or tubular damage that destroys individual nephrons interstitial nephritis
(1) the inability of the bladder to empty completely, leaving residual urine in the bladder (2) the existence of obstruction of urine outflow. impaired ability to flush bacteria from the bladder becomes inflamed, a condition termed cystitis. Bacteria may reach the renal pelvis This condition is called vesicoureteral reflux and is due to the failure of the bladder wall to occlude the ureter during micturition Initiate the infection and inflammation associated with pyelonephritis Affect medulla first ----> impair renal ability to concentrate urine Finally whole renal damage occurs
Changes in nephron functions with renal failure Water and solute excretion: Patients who have lost up to 75 to 80 % of their nephrons are able to excrete normal amounts of water and electrolytes without serious accumulation of any of these in the body fluids. Further reduction in the number of nephrons, however, leads to electrolyte and fluid retention When the number of nephrons falls below 5 to 10 % of normal ----> death occurs.
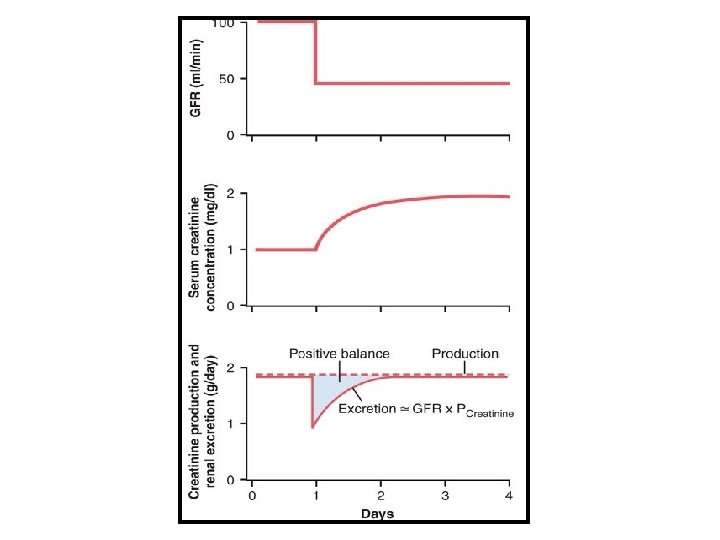
In contrast, waste products of metabolism, such as urea and creatinine, accumulate almost in proportion to the number of nephrons that have been destroyed. Why? substances such as creatinine and urea depend largely on glomerular filtration for their excretion, and they are not reabsorbed as avidly as the electrolytes. Creatinine, for example, is not reabsorbed at all, and the excretion rate is approximately equal to the rate at which it is filtered.
if GFR decreases, the creatinine excretion rate also transiently decreases, causing accumulation of creatinine in the body fluids and raising plasma concentration until the excretion rate of creatinine returns to normal Thus, under steady-state conditions the creatinine excretion rate equals the rate of creatinine production, despite reductions in GFR; however, this normal rate of creatinine excretion occurs at the expense of elevated plasma creatinine concentration
In the case of sodium and chloride ions, their plasma concentrations are maintained virtually constant even with severe decreases in GFR. This is accomplished by greatly decreasing tubular reabsorption of these electrolytes.
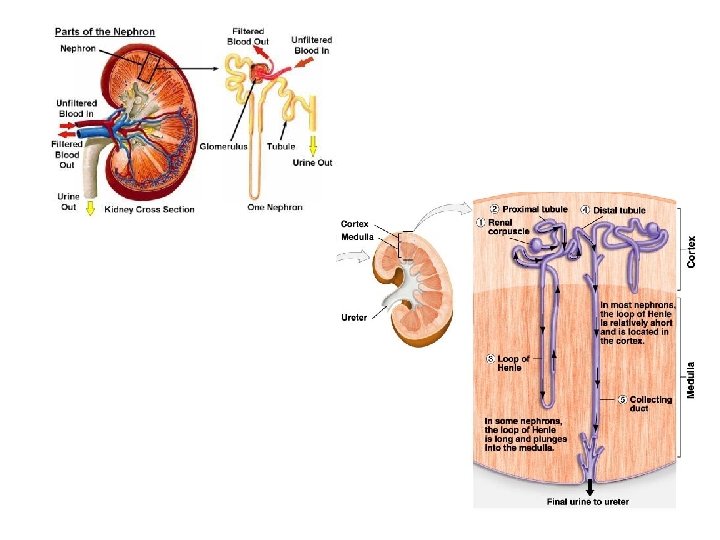
Inability of the Kidney to Concentrate or Dilute the Urine = Isosthenuria The concentrating ability of the kidney is impaired mainly because (1)the rapid flow of tubular fluid through the collecting ducts prevents adequate water reabsorption, and (2)the rapid flow through both the loop of Henle and the collecting ducts prevents the countercurrent mechanism from operating effectively to concentrate the medullary interstitial fluid solutes.
Therefore, as progressively more nephrons are destroyed, the maximum concentrating ability of the kidney declines and urine osmolarity and specific gravity (a measure of the total solute concentration) approach the osmolarity and specific gravity of the glomerular filtrate.
The diluting mechanism in the kidney is also impaired when the number of nephrons decreases because the rapid flushing of fluid through the loops of Henle and the high load of solutes such as urea cause a relatively high solute concentration in the tubular fluid of this part of the nephron. As a consequence, the diluting capacity of the kidney is impaired and the minimal urine osmolality and specific gravity approach those of the glomerular filtrate.
The effect of renal failure on the body fluids depends on (1) water and food intake and (2) the degree of impairment of renal function. 1) generalized edema resulting from water and salt retention; (2) acidosis resulting from failure of the kidneys to rid the body of normal acidic products; (3) high concentration of the nonprotein nitrogens-especially urea, creatinine, and uric acid-resulting from failure of the body to excrete the metabolic end products of proteins; and (4) high concentrations of other substances excreted by the kidney, including phenols, sulfates, phosphates, potassium, and guanidine bases.
This total condition is called uremia because of the high concentration of urea in the body fluids.
Thank you