NANTAI NVERSTES CLINICAL PSYCHOLOGY DIAGNOSIS IN CLINICAL PSYCHOLOGY










")

 Ensures comparability among identified patients Promotes research")

. 1.")
- Slides: 17
NİŞANTAŞI ÜNİVERSİTESİ CLINICAL PSYCHOLOGY DIAGNOSIS IN CLINICAL PSYCHOLOGY İktisadi, İdari ve Sosyal Bilimler Fakültesi iisbf. nisantasi. edu. tr NİŞANTAŞI ÜNİVERSİTESİ ©
WHAT IS ABNORMAL BEHAVIOR? No single descriptive feature is shared by all forms of abnormal behavior, and no one criterion for “abnormality” is sufficient. No discrete boundary exists between normal and abnormal behavior. Many individuals still equate abnormal behavior with (a) bizarre behavior, (b) dangerous behavior, or (c) shameful behavior. Three proposed definitions of abnormal behavior: (a) statistical infrequency or violation of social norms, (b) the experience of subjective distress, (c) disability, dysfunction, or impairment.
The Rosenhan Study: On Being Sane in Insane Places
Assessment is the systematic evaluation and measurement of psychological, biological, and social factors in an individual presenting with a possible psychological disorder. Diagnosis is the process of determining whether the presenting problem(s) fit the criteria for a particular mental disorder.
Clinical Diagnosis Aims to fully understand the client. Aids in understanding and curing human suffering. Why diagnose? To define typical symptom cluster, natural history and causes To determine treatment Based on reliable, valid, and standardized information
Two Widely Used Classification Systems ICD-10 International Classification of Diseases and Health Related Problems (ICD-10) Published by the World Health Organization DSM-IV & DSM-IV-TR & DSM-5 Diagnostic and Statistical Manual of Mental Disorders
The purpose of DIAGNOSTIC SYSTEM gives us a reliable picture of the person we are dealing with… DSM –I 1952. DSM-II 1968. DSM –III- 1980 DSM-III-TR- 1987 DSM IV 1994. DSM IV-TR 2000 DSM-5 2013
The DSM- IV Basic Characteristics • Five axes • Full clinical presentation • Clear inclusion and exclusion criteria for disorders • Disorders are categorized under broad headings • Empirically-grounded, prototypic approach to classification
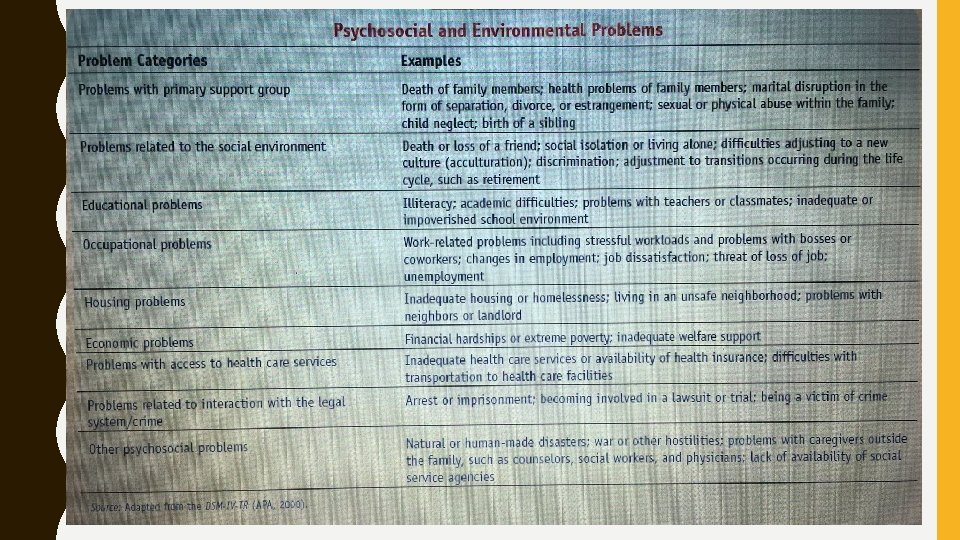
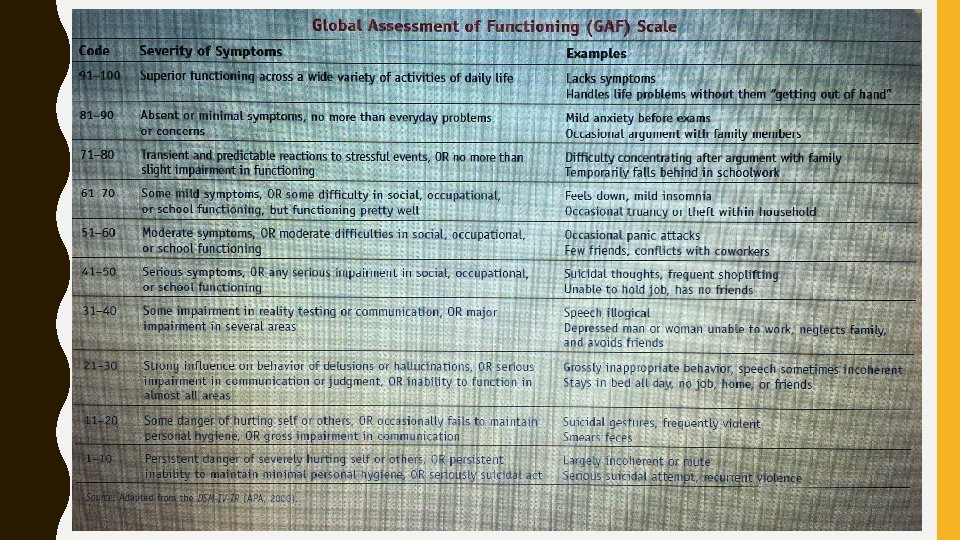
The Five DSM-IV Axes § Axis I : Clinical Disorders or Other Conditions That May Be a Focus of Clinical Attention § Axis II: Personality Disorders § Axis III: General Medical Conditions That Are Potentially Relevant to the Understanding or Management of the Individual’s Mental Disorder § Axis IV : Psychosocial and Environmental Problems § Axis V : Global Assessment of Functioning (GAF) Scale
The Case of Michelle M. was a 23 -year-old woman admitted to an inpatient unit at a hospital following her sixth suicide attempt in 2 years. She told her ex-boyfriend (who had broken up with her a week earlier) that she had swallowed a bottle of aspirin, and he rushed her to the local emergency room. Michelle had a 5 -year history of multiple depressive symptoms that never abated; however, these had not been severe enough to necessitate hospitalization or treatment. They included dysphoric mood, poor appetite, low self-esteem, poor concentration, and feelings of hopelessness. In addition, Michelle had a history of a number of rather severe problems that had been present since her teenage years. First, she had great difficulty controlling her emotions. She was prone to become intensely dysphoric, irritable, or anxious almost at a moment’s notice. These intense negative affect states were often unpredictable and, although frequent, rarely lasted more than 4 or 5 hours. Michelle also reported a long history of impulsive behaviors, including polysubstance abuse, excessive promiscuity (an average of about 30 different sexual partners a year), and binge eating. Her anger was unpredictable and quite intense. For example, she once used a hammer to literally smash a wall to pieces following a bad grade on a test. Michelle’s relationships with her friends, boyfriends, and parents were intense and unstable. People who spent time with her frequently complained that she would often be angry with them and devalue them for no apparent reason. She also constantly reported an intense fear that others (including her parents) might abandon her. For example, she once clutched a friend’s leg and was dragged out the door to her friend’s car while Michelle tried to convince the friend to stay for dinner. In addition, she had attempted to leave home and attend college in nearby cities on four occasions. Each time, she returned home within a few weeks. Prior to her hospital admission, her words to her exboyfriend over the telephone were, “I want to end it all. No one loves me. ”
Diagnostic Evaluation of Michelle M. According to DSM-IV Axis I: Dysthymic Disorder (early onset) Alcohol Abuse Cannabis Abuse Cocaine Abuse Hallucinogen Abuse Axis II: Borderline Personality Disorder (PRINCIPAL DIAGNOSIS) Axis III: none Axis IV: Problems with primary support group Educational problems
DSM 5 Axis I: Clinical Disorders This is the top-level of the DSM multiaxial system of diagnosis. It represents acute symptoms that need treatment; Axis I diagnoses are the most familiar and widely recognized (e. g. , major depressive episode, schizophrenic episode, panic attack). Axis II - Personality Disorders and Intellectual disabilities Axis II is for assessing personality disorders and intellectual disabilities. These disorders are usually life-long problems that first arise in childhood, distinct from the clinical disorders of Axis I which are often symptomatic of Axis III - General Medical Conditions Axis III describes physical problems that may be relevant to diagnosing and treating mental disorders. Note: General medical conditions can be regarded in basically three ways. ● First, as being directly related to mental disorders; ● Second, as being important to the overall diagnostic picture; ● Third, as not having a sufficient relationship. Important Note: American Psychiatric Association. (2014). Highlights of Changes From DSM-4 -TR to DSM-5. American Psychiatric Publication.
Diagnosis: Positive Aspects Facilitates communication (verbal shorthand) Ensures comparability among identified patients Promotes research on diagnostic features, etiology and treatment Diagnosis: Negative Aspects • Boundaries between disorders are often fuzzy • Negative effects of labeling on other’s perceptions • Negative effects of labeling on self-concept
Ethnic and Cultural Considerations Culture may influence expression of illness. Individuals have a right to define their culture. • • Pathology must be diagnosed within a cultural context.
REFERENCES Clinical Psychology, Timothy J. Trull - Mitchell J. Prinstein, Wadsworth Publishing, (2012). 1. Introduction To Clinical Psychology / Seventh Edition by Geoffrey P. Kramer, Douglas A. Bernstein, Vicky Phares 2. Clinical Psychology: A Modern Health Profession / 1 st Edition by Wolfgang Linden , Paul Hewitt - Nobel 3. American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders (4 th ed. , text rev. ). Washington, DC. 4. American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5 th ed. ). Washington, DC. 5. American Psychiatric Association. (2014). Highlights of Changes From DSM-4 -TR to DSM-5. American Psychiatric Publication. 6. Köroğlu, E. (2013). DSM-5 Tani Ölçütleri. Ankara: Boylam Psikiyatri Enstitüsü. 7. Öztürk, O. (2014). DSM-5 Türkçe Çevirisi Üzerine. Türk Psikiyatri Dergisi 8. NİŞANTAŞI ÜNİVERSİTESİ ©