Complications in orthopaedics Teerakorn wongwises MD Objective 1

Complications in orthopaedics Teerakorn wongwises MD.

Objective 1. Meaning. 2. Principal of Rx. 3. Knowledge & management I. III. IV. Fat embolism syndrome Crush syndrome Acute compartment syndrome Pin tract infections 4. Communication technique

Complications An additional diagnosis describing a condition arising after beginning of hospital observation and treatment , thus modifying the course of the patient’s illness or the medical care required. Noun Orthopaedic dictionary

Systemic complications VS Local complications Early VS late Preventable VS Inevitable

Principal of Rx 1. Save life 2. Save limb 3. Preserve function 4. Improve cosmetic

Save life ATLS Primary servey ABCD Re-evaluation Improved Not improved To 2 nd servey

Save limb Blood supply Muscle Nerves Tendons Bone

Preserve function Painless Stable joint Solid union

How to Diagnosis ü History taking ü Physical examination ü Investigation – Blood – Radiographic : plain film , CT , MRI , bone scan, etc.

Limitations v. Unconsciousness v. Co morbidity : HI , Nerve injury v. Child v. Language
ARDS")
Systemic Complications üFat embolism syndrome o Respiratory failure and adult respiratory distress syndrome )ARDS ( üCrush syndrome

Local Complications üAcute compartment syndrome üPin tract infections

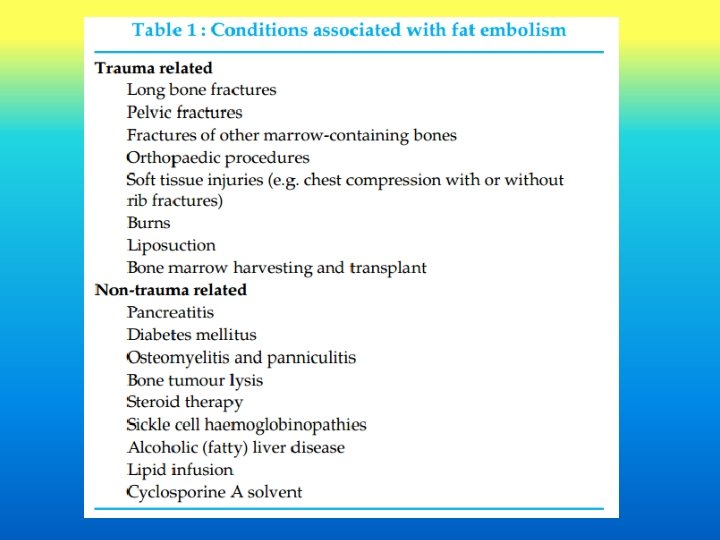
Fat Embolism Syndrome / FES The presence of fat globules in the peripheral circulation and lung parenchyma after fracture of long bones, pelvis or other major trauma. Zenker ***1861
![Fat Embolism Syndrome / FES Clinical diagnosis [ Bergmann *** 1873 ] Dyspnoea Petechiae](http://slidetodoc.com/presentation_image_h/cbb3ab0c9be062b0f901fa591aa1346b/image-14.jpg "Fat Embolism Syndrome / FES Clinical diagnosis [ Bergmann *** 1873 ] Dyspnoea Petechiae")
Fat Embolism Syndrome / FES Clinical diagnosis [ Bergmann *** 1873 ] Dyspnoea Petechiae mental confusion

Fat Embolism Syndrome q. Incidence v. Most commonly is associated with long bone and pelvic fractures v. Closed > opened v. Higher in young men but rarely in child

Fat Embolism Syndrome q. Causes v. Skeletal injury / trauma related v. Non-traumatic conditions DM, pancreatitis

Pathophysiology 1. The Mechanical theory 2. Biochemical theory 3. Coagulation theory

Clinical Features q. Delay presents 12 -72 hrs after the initial injury q. Classic triad of : – respiratory manifestations (95%) • Dyspnoea, tachypnoea and hypoxaemia • Respiratory failure – cerebral effects (60%) • Present in the early stages • Wide spectrum from mild confusion and drowsiness through to severe seizures. • +/- focal neurological signs – petechiae (33%). • may be the last • conjunctiva, oral mucous membrane and skin folds of the upper body especially the neck and axilla.

Clinical Features cont’ • Ocular manifestation – Purtscher’s retinopathy • CVS involvement – Early persistent tachycardia • Systemic fever

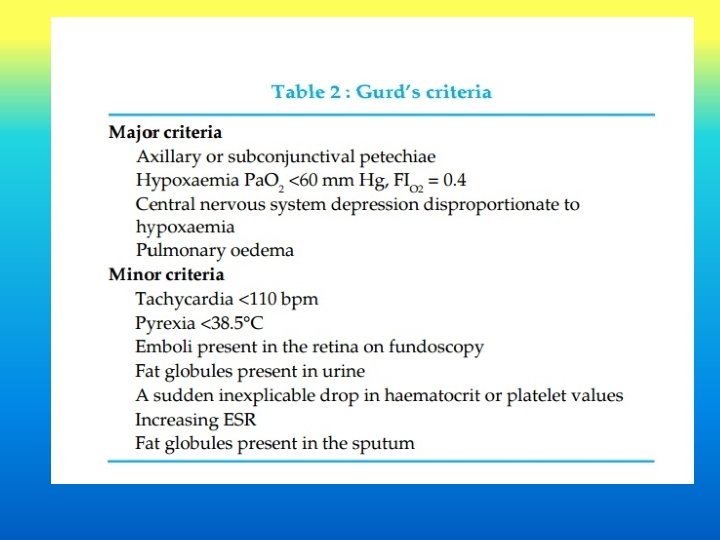
Diagnosis v. Base on clinical findings. v. Gurd’s criteria at least 1 major and 4 minor criteria v. Lindeque’s criteria

Lindeque’s criteria • • Fat embolism index Semi-quantitative means of diagnosis 7 clinical features Score of >5 is required for a positive diagnosis. Ref : Schonfeld SA, et al. Fat embolism prophylaxis with corticosteroids. Ann Intern Med 1983

Investigations • To support the clinical diagnosis or to monitor therapy • Hematology and Biochemistry – Anemia and thrombocytopenia – Hypocalcemia – Hypofibrinogenemia – raised ESR – prolongation of Prothrombin time

Investigations • Urine and Sputum examination • Arterial blood gases • Chest X-ray snow storm appearance • Lungs scan may show ventilation perfusion mismatch. • EKG , Transesophageal echocardiography • Bronchoalveolar lavage • CT / MRI Brain

Treatment üMedical Care üSurgical Care üProphylactic treatment

Medical Care Adequate oxygenation and ventilation Stable hemodynamics Hydration Prophylaxis of deep venous thrombosis Stress related gastrointestinal bleeding and nutrition. • Drugs ***inconclusive results*** • • • supportive treatment

Drugs Corticosteroids Aspirin Heparin N-Acetylcysteine
 of 50 –")
supportive treatment 1. Spontaneous ventilation FIO 2 (inspired O 2 concentration) of 50 – 80%. 2. CPAP and noninvasive ventilation added to improve Pa. O 2 3. Mechanical ventilation and PEEP

Surgical Care • Early immobilization • Operative VS Conservative • Limit the elevation in intraosseous pressure during orthopaedic procedures

Prophylactic treatment • Albumin – Restores blood volume – Binds fatty acids and may decrease the extent of lung injury. Ref ; MG Abbott. Fat embolism syndrome : An in-depth review. Asian Journal of Critical Care 2005 • Corticosteroid – Controversial / no significant changes in mortality Methylprednisolone 1. 5 mg kg-1 i. v. every 8 h for 6 doses.

Prognosis Mortality is estimated to be 5 -15% overall but most patients will recover fully.

Crush Injury and Crush Syndrome v. Crush injury is a direct injury resulting from crush. v. Crush syndrome is the systemic manifestation of muscle cell damage resulting from pressure or crushing. 1941 / Bywaters and Beall vnatural or manmade disaster

Pathogenesis and Clinical Features muscle cell injury leak contents out of the cells into the circulation – Myoglobin )nephrotoxic( – urate and phosphate )nephrotoxic( – potassium )cardiotoxic (

Pathogenesis and Clinical Features muscle cell injury allows passage of water , calcium, and sodium into the cells from the extracellular space muscle swelling and intravascular volume depletion and resulting in hypovolemic shock.
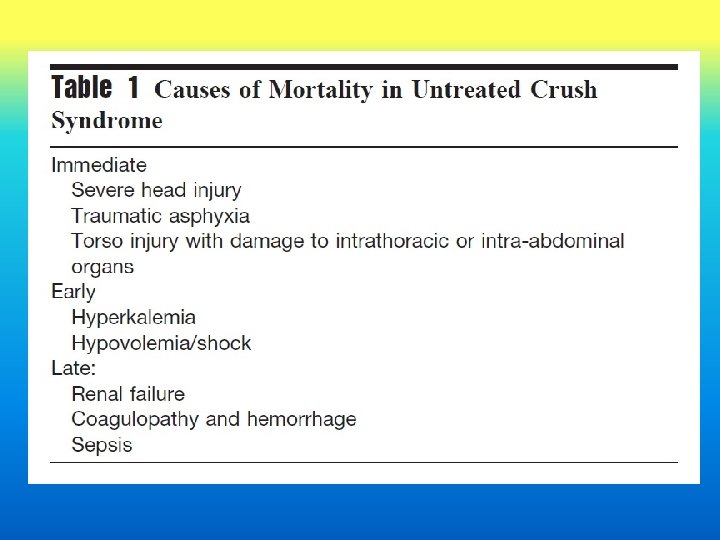

Cardiovascular instability Commonly / multifactorial ühypovolemic shock ümyocardial toxicity from the associated electrolyte disturbance

Renal failure v. Most serious / multifactorial v. Vasomotor and nephrotoxic elements Myoglobin, urate, and phosphate distal convoluted tubules and tubular cast formation tubular obstruction.
 • Correlate with development of renal failure and mortality. •")
Peak creatine kinase (CK) • Correlate with development of renal failure and mortality. • peak CK 75, 000 U/L. • Oda et al. number of crushed limbs ***more practical and immediate estimate of the severity of impending crush syndrome. • Crush to one, two, and three extremities led to an incidence of renal failure of 50%, 75%, and 100%, respectively.

Management v. Pre hospital üABCD + associated injury üOxygen ücontrolled hemorrhage üIntravenous access + fluid

Management v. In hospital ücatheterized and hourly urine üElectrolytes, arterial blood gases , and muscle enzymes should be measured. üCentral venous pressure monitoring.

Fluid Physiologic normal saline large volumes § 200 m. L of potassium free solution per hour § target urine output of at least 8 L/day § level of hydration / CVP monitoring Alkalinization / sodium bicarbonate Mannitol / benefit up to 48 hours after injury 1 to 2 g/kg over the first 4 hours )20%solution(

Compartment syndrome q. Uptake of fluid into muscle cells contained within a tight compartment. q. Controversial Rx ? ? Mannitol / fasciotomy

Compartment syndrome üAcute compartment syndrome o Chronic exertional compartment syndrome

Acute compartment syndrome Compartment syndrome as an elevation of the interstitial pressure in a closed osseofascial compartment that results microvascular compromise, tissue ischemia, necrosis, and functional impairment Volkmann's ischemic contracture Mubarak

EPIDEMIOLOGY
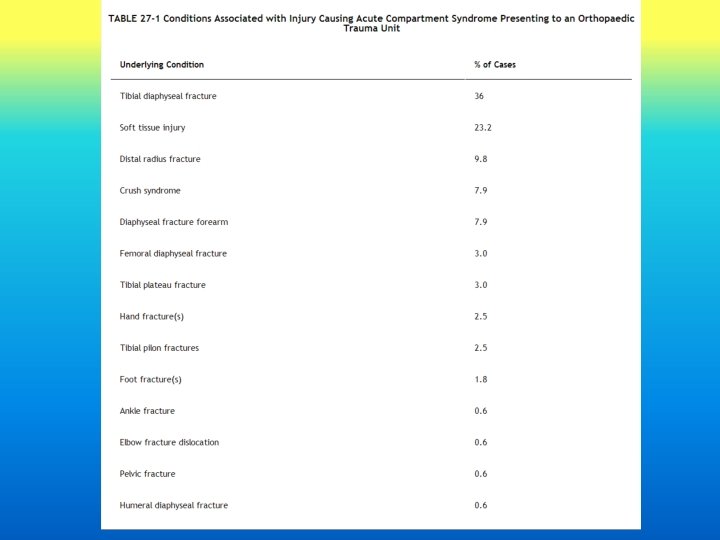

Diagnosis I. II. Clinical diagnosis Compartmental pressure monitoring

Clinical diagnosis 1948, Griffiths described four main symptoms of a manifest compartment syndrome: pain, paresthesia, paresis and pain with stretch ( the ‘‘four Ps. ( Pain was identified as the earliest and most sensitive clinical sign of a manifest compartment syndrome. Early recognition most important

Clinical diagnosis The most important sign is pain out of proportion to that expected with the injury Pain with passive stretch had comparable sensitivity , specificity , and predictive values.

Compartmental Pressure Monitoring Tissue pressure / relative tissue pressure Tissue pressure 30 -50 mm Hg

Compartmental Pressure Monitoring Whitesides : difference between the diastolic blood pressure and tissue pressure = ΔP Tissue pressure rises to within 10 to 30 mm Hg of the diastolic pressure Persistent ΔP of less than 30 mm Hg => fasciotomy

J Trauma. 2006; 60: 1037– 1040.

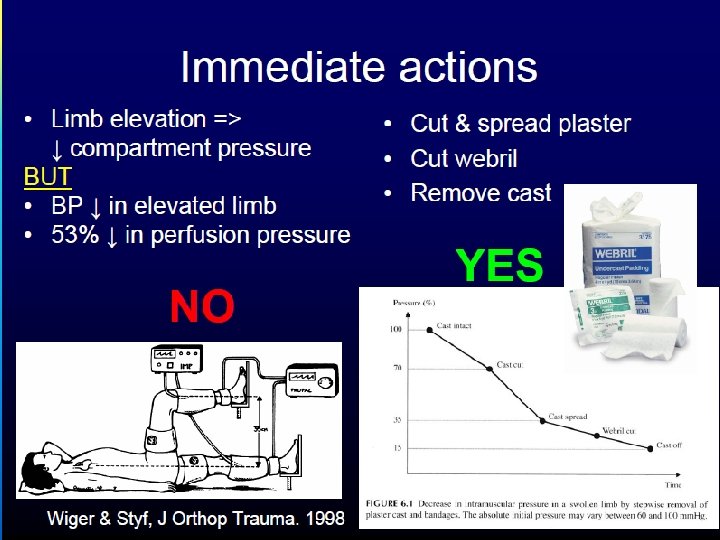
Treatment Immediate Rx üRelease of external limiting envelopes such as dressings or plaster casts üLimb should not be elevated above the height of the heart üCorrected hypotension üOxygen therapy

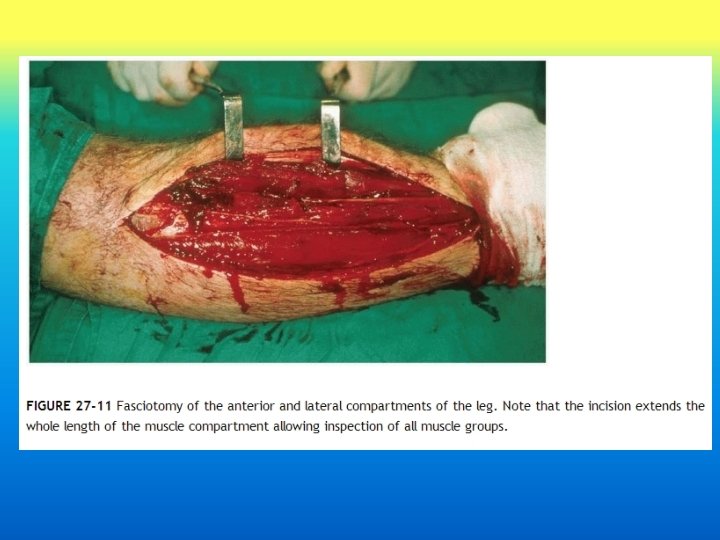
Treatment Fasciotomy *** time ***

Rockwood and Green’s 8 th ed.

Rockwood and Green’s 8 th ed.

Pin tract infection Incidence from 11. 3% to 100%. N Ferreira et. al Failure of the bone-pin interface üPin loossening üFailure of construct üMalalignment / malunion Chronic osteomyelitis Sepsis

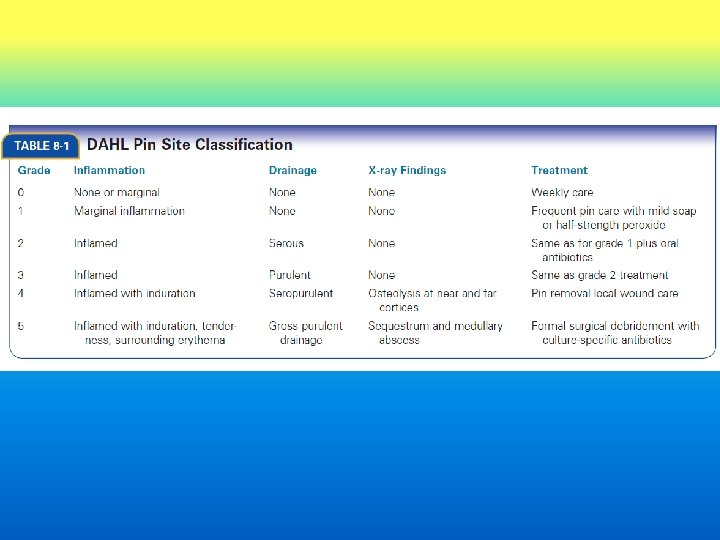
Classification Rockwood and Green’s 8 th ed.

Pin Care no consensus Researchers concluded that evidence was insufficient to recommend a specific technique to minimize infection and prevent complications. AMERICAN JOURNAL OF CRITICAL CARE, July 2012, Volume 21, No. 4

Pin Care ? ? ? frequency daily / weekly Cleansing solutions …. Dressing ? ? Showering ? ? Crusts removal ? ? ABO Ointment. Sterile / clean technique. Patient education.

Frequency • Immediate postoperative – compressive dressing **stabilize the pin–skin interface and minimize pin–skin motion – 10 days to 2 weeks Rockwood and Green’s 8 th ed. • After skin healing – daily / weekly

Santy JE, et al. The Rubber Stopper: A Simple and Inexpensive Technique to Prevent Pin Tract Infection following Kirschner Wiring of Supracondylar Fractures of Humerus in Children Malaysian Orthopaedic Journal 2015 Vol 9 No 2

Cleansing solutions ü Chlorhexidine 2 mg/ml ü 0. 9% Na. Cl ü Half-strength hydrogen peroxide solutions Rockwood and Green’s 8 th ed. ü 70% alcohol ü Betadine solution ** interferes tissue healing Kramer SA. Effect of povidone-iodine on wound healing: a review. J Vasc Nurs. 2000; 17(1): 17 -23. ü Mild soap and water

Dressing Immediate postoperative

Dressing After skin healing

Showering Daily showers , water flow => no major infection Gordon, et al. Pin site care during external fixation in children: Journal of Pediatric Orthopaedics, 20(2), 163– 165. After 5 to 10 days. / United States and Europe Covering of the fixator during showering. W-Dahl A, et al. Pin site care in external fixation sodium chloride or chlorhexidine solution as a cleansing agent. Arch Orthop Trauma Surg. 2004; 124(8): 555 -558.

Crusts removal ? ?

Crusts removal ? ? ü Recommendations =>remove the crusted material ü Stiffen the pin–skin interface and increase shear forces at the pin–bone interface ü Development of additional necrotic tissues and fluid buildup around the pin Clasper JC, et al. Fluid accumulation and the rapid spread of bacteria in the pathogenesis of external fixator pin track infection. Injury. 2001; 32(5): 377– 381. Rockwood and Green’s 8 th ed.

ABO Ointment Not recommended for postcleansing care, as these tend to inhibit the normal skin flora and can lead to superinfection or pin site colonization Marotta JS, et al. Long-term bactericidal properties of a gentamicincoated antimicrobial external fixation pin sleeve. J Bone Joint Surg Am. 2003; 85 -A( Suppl 4): 129– 131. Rockwood and Green’s 8 th ed

Sterile VS clean technique üIn hospital *** sterile üAt home / self – care*** clean Holmes, S. & Brown, S. (2005). Skeletal pin site care: National Association of Orthopaedic Nursing guidelines for orthopaedic nursing. Orthopaedic Nursing, 24(2), 99 -107

Patient education Recommend § Patient/family demonstration of pin site care before leaving the hospital. § Written instructions for site care. § Written description of the early signs of infection and a loose pin. § Information about how to contact the orthopaedic team. W-Dahl A, et al. Pin site care in external fixation sodium chloride or chlorhexidine solution as a cleansing agent. Arch Orthop Trauma Surg. 2004; 124(8): 555 -558.

Orthopedic pin-care protocol from Hennepin County Medical Center. in Minneapolis, Minnesota Classifies pin-site appearance and indicates the appropriate care. No redness or drainage => weekly cleansing with normal saline Slightly red => cleansing with normal saline Red and tender with a colorless watery or clear yellow drainage => cleansing with half-strength H 2 O 2 Worsening redness, draining, or swelling => back to orthopedic clinic to start antibiotics.

Complications ≈ Bad news

Dr. Elisabeth Kübler-Ross • Swiss psychiatrist • On Death and Dying • 1969

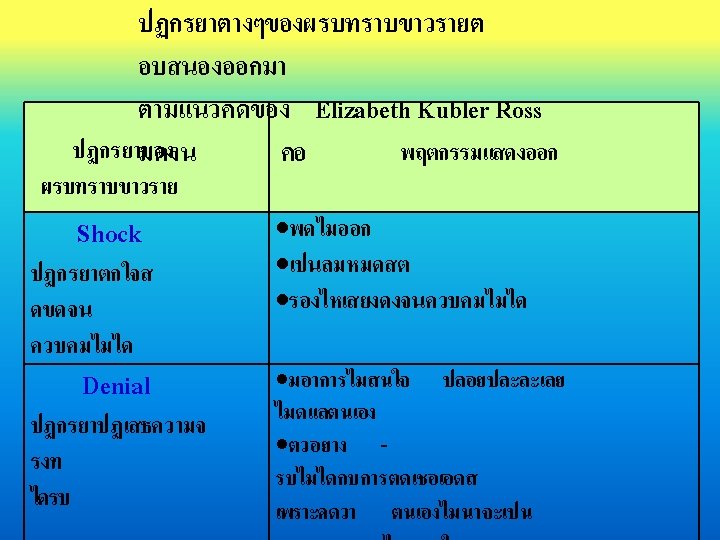
Kubler. Ross Theory ปฏกรยาการแสดงออกเมอทรา บขาวราย Acceptance Denial Depression Anger Bargaining 37

การแจงขาวราย SPIKES model f o r breaking bad news Setting up the interview Perception of the patient Invitation by the patient Knowledge to the patient Emotions of the patient Strategy and summary


 38% : vocal (volume,")
การสอสาร ผพด ผฟง Impact on listener 7% : verbal (words) 38% : vocal (volume, pitch, rhythm, etc) 55% : body language

Body Language • Face: expression, smile, head • Figure: posture, clothes, hand • Focus: eye contact, distraction material • Territory: personal space
- Slides: 90