HIRSCHSPRUNGS DISEASE Hirschsprungs disease is also called as








 of the abnormal")






- Slides: 16
HIRSCHSPRUNG’S DISEASE
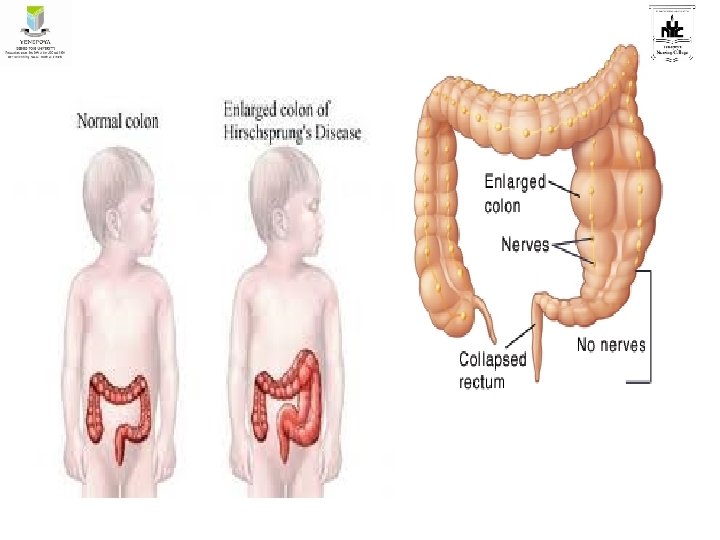
• Hirschsprung’s disease is also called as congenital aganglionic megacolon. • It occurs due to congenital absence of the parasympathetic ganglionic nerve cells , both in muscle layer or submucosal layer of distal colon or rectum, which results in extreme dilation of the colon. • It involves varying lengths and even the whole of the colon. • Most commonly affected part is the rectosigmoid colon.
• Etiology is unknown • Found as familial illness with genetic predisposition. • Commonly found in male child • Found about 1 in 5, 000 births.
PATHOPHYSIOLOGY: • The disease develops due to an arrest in embryonic development affecting the migration of parasympathetic nerves in the intestine occurring before the 12 th week of gestation. • The intrinsic ganglion cells are absent in muscle layer and in submucosal layer of the intestine. • These results in lack of coordination of the peristalsis causing functional obstruction with dilatation and hypertrophy of the proximal normal ganglionic colon.
• No peristalsis occurs in the affected part and it becomes spastic, contracted and narrowed. So no faecal material passes through it, thus leading to the accumulation of faecal material above the affected portion. • The colon, proximal to the narrow affected part, is dilated and filled up with fecal material and gases. • Ulceration of mucosal layer may develop especially in neonates. • Evacuation of fecal material and gases is prevented due to failure of internal rectal sphincter to relax, resulting in abdominal distension and constipation.
CLINICAL MANIFESTATIONS: • Clinical manifestations depend upon the degree of involved part. • In neonates symptoms appear within 7 days. ü Delayed passage of meconium. ü Bile stained or fecal vomiting ü Abdominal distension and constipation ü Some times overflow type of diarrhoea and dehydration ü Neonates may present with features of intestinal obstruction and failure to thrive
• In older children, the symptoms are not prominent at birth. ü History of intractable constipation ü Progressive abdominal distension ü Visible peristaltic activity. ü Anorexia, abdominal discomfort, irritability, constipation unresponsive to conventional remedies. ü Absence of will to defecate ü Diarrhoea alternating with constipation and presenting as ribbon like, fluid like or pellete stools. ü Child may complicate with gross malnutrition, anemia and failure to thrive.
DIAGNOSIS: • History • Physical examination • Rectal examination which reveals a tight anal sphincter, and empty rectum followed by an explosive gush of stool and flatus. • Plain X-Ray abdomen • Barium enema • Ano-rectal manometry • Biopsy of rectal and colonic tissue
Management: • Treatment of Hirschsprung's disease consists of surgical removal (resection) of the abnormal section of the colon, followed by reanastomosis. • Colostomy The first stage of treatment used to be a reversible colostomy. In this approach, the healthy end of the large intestine is cut and attached to an opening created on the front of the abdomen. The contents of the bowel are discharged through the hole in the abdomen and into a bag. Later, when the child’s weight, age, and condition is right, the "new" functional end of the bowel is connected with the anus.
• The reconstructive surgery is done by following 3 techniques. ü Swenson pull-through surgery: . ü Duhamel procedure ü The Soave procedure
• The optimal age for these surgeries is 6 -8 months after temporary colostomy or 12 -15 months of age or until the child’s weight is 7 -9 Kg. • In older children where the symptoms are not severe management should be done by repeated enemas with isotonic saline, stool softeners and low residual diet.
Complications: • Enterocolitis • Bowel perforation • Intestinal obstruction • Hydroureter or hydronephrosis • Failure to thrive • Nutritional deficiencies
Post operative complications: • Enterocolitis • Leaking of anastamosis • Colostomy related problems • Pelvic abscesses • Temporary constipation • Intestinal obstruction • Infections • Haemorrhage • Shock
Reference • Hockenberry, Wilson, Judie. Wong’s essentials of pediatric Nursing. South India Edition. Elsevier publication. • Dorothy R Marlow, Barbara A Redding, Raman Kalia. Marlow’s textbook of pediatric Nursing. Harcourt Brace & Company Asia Pte Ltd. • Parul Datta. Pediatric Nursing. 4 th edition. Jaypee Publishers. New Delhi.
THANK YOU