Greater Manchester Early Years Speech Language and Communication






















- Slides: 23
Greater Manchester Early Years Speech, Language and Communication Pathway and Specification Michelle Morris Consultant SLT Salford Royal (NHS) Foundation Trust
Greater Manchester Heath and Social Care Partnership Facts and Figures • • Covers 10 LA areas 37 NHS organisations and councils Population: 2. 8 million Budget: £ 6 billion School readiness ê than nat. av. for GLD (62. 4%) GM av. 62. 4% (range 73. 4 -57. 2%) 2 in 5 don’t reach GLD. é 1 in 2 for children on FSM |1
Devolution Manchester or as we call it Devo Manc. GM: 1 st region to receive delegated power from central government to local area • 2014: new powers transport, housing, planning and policing. • 2016 Take over the health and social care budget • Opportunity to tackle the health inequalities • GM received 450 million additional transformation funding • 2017 Election of a region Mayor today! 2
The Plan -Taking Charge 20162021 5 year plan to deliver: • 1, 300 fewer people dying from cancer • 600 fewer people dying from cardiovascular disease • 580 fewer people dying from respiratory disease • 270 more babies being é 2, 500 g making difference to long term health • Supporting people to stay well and live at home for as long as possible, with 2, 750 fewer people suffering serious falls • More children reaching a good level of social and emotional development with 3, 250 more children ready for the start of school aged 5 (other outcomes being developed) |3
GM Start Well: Early Years Strategy • The ambition: every child acquires the skills necessary to negotiate early childhood , primary and secondary education and employment. • Sets out the GM transformational vision for system change • Shift from expensive reactive public services to prevention and early intervention • Acknowledges the diverse range of stakeholders in EY system • Sets out a host of additional outcome for children • Strengthening universal and targeted services
Start Well cont … • • Break the cycle of poverty Develop a consistent approach to delivery Underpinned by integrated commissioning Strengthening family and community capacity for managing own health and well being • Recognition that cost benefits wont be realised for at least 10 years |5
Healthy Child Programme Mandated Contacts • • • Anti natal New baby review 6 -8 week assessment 1 yr. assessment 2 -2. 5 year review |6
|7
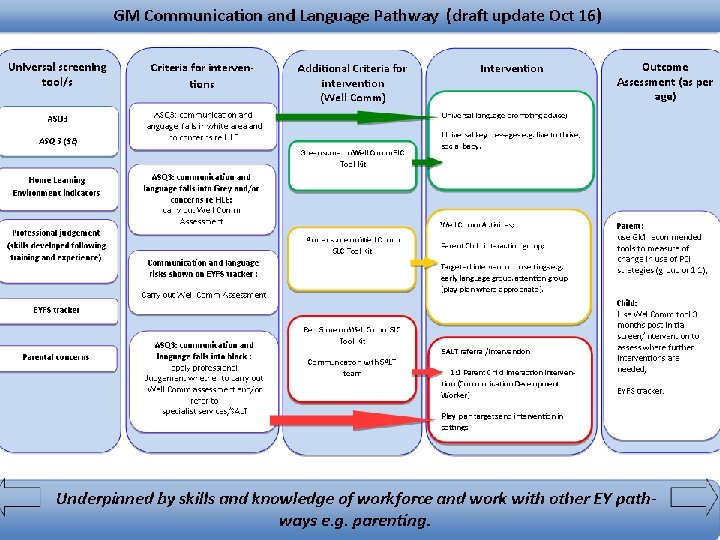
Key Features: GM 8 Stage Model • Systematic surveillance using ASQ 3. • Introduced a recommended Level 4 b assessment at 18 months. 2 years considered too late • Feedback: Very important for identifying SLCN. • ASQ 3 (Developmental) largely on parental report • ASQ (SE) Social Emotional. GM recommended for use at stages 4 - 8 • Is ASQ accurate at identifying SLCN? • Produces a risk rating White/Grey/Black • Integrate delivery: CC workers and HV team. • Increase the sensitivity of SLC assessment by introduction of Wellcomm. |8
SLCN pathway background • 2012 - developed a multi agency SLCN delivery pathway in Salford based on best available evidence and commissioned by the LA and PCT • 2014 – Asked to lead a small project group to develop a pathway based on the existing good practice. This formed the 1 st GM pathway & specification and pathway. Much of the work was already tested and had demonstrated effectiveness. Pathway developed over 2014 • 2016: Work to refresh and update the pathway & specification with wider group of stakeholders. Supported by senior GM programme manager |9
Specification • Identified required outcomes • Different levels of intervention • Communication and Language is embedded in all aspects of – Planning – Work with parents • Requirement for partnership working • Evidence based interventions for supporting families • Identifies the support required from SLT team • Workforce Development | 11
Workforce Development • Every team and setting has a Communication Lead • Level of competency for different roles • Rolling programme of training to develop universal and enhanced level competencies in SLC based on SLCF. • Recognising need for access to ongoing support and advice for staff from specialists | 12
Wellcomm • Evidence based screening tool. • Developed by Sandwell & West Birmingham NHS Hospital Trust’s SLTs service in 2010 rev. 2015 • Split into 9 stages from 6 m to 6 years • Asks 10 questions plus narrative • Direct observation, assessment and discussion with family – Eg 18 -23 m: 50% parental report – 24 -29 m: 20 % parent report | 13
Wellcomm Cont …… • Quick and easy to administer • Basic training required but can be administered by a wide range of staff. Precondition of use, universal level competencies. • Provides a profile & RAG rates children at risk • Provides clear simple intervention strategies | 14
Case study 1 Child A • Scored secure white at 26 months on ASQ • CNN had concerns used professional judgement and assessed on Wellcomm • Child screened as RED on Wellcomm • Wellcomm activities given to parents. Child referred to SALT • Assessed and advice given placed on CDW waiting list. • CDW commenced visits for individualised PCI and lang stimulation strategies. • Parents already using Wellcomm strategies & advice from SLT • Parents could see progress being made • CDW modelled further strategies which parent is now using. • Child will be reviewed in clinic following CDW visits | 15
Case study 2 child H • • • Scored grey on ASQ @ 2 yr developmental check Referred to Talking Tots (PCI group) Referrer highlighted unclear speech Child very chatty , sociable Wellcomm pre intervention: Amber with delay in expressive language. • Family and referrer surprised as so chatty • Family attended TT and received intervention in setting awaiting post intervention Wellcomm. | 16
What we know so far • Wellcomm does highlight Amber children who go on to access targeted interventions e. g. PCI, Wellcomm activities and Stay and Play • More children referred directly to SLT • Pathway is highlighting previously unmet targeted and specialist need • Example Locality W • 61 children identified on ASQ as requiring Wellcomm in 6 m period 8% Green : 70% Amber: 22% Red | 17
Key learning • Setting the standard but allowing for flexibility in local provision • The importance of developing a shared culture • Using a common language • Developing shared outcomes • The importance of enablers like info systems | 18
Next steps • Developing a communication strategy • Collecting data on improved identification with a view to a GM business case • Standardising more packages of training e. g. Wellcomm introduction • Getting rid of DNA discharge for clinical services • Rolling out the Manchester developed training for childminders | 19
Challenges • • • Encouraging consistency Data collection and sharing: different systems/rules How do we hold authorities to account? Managing preconceptions Ensuring programmes are linked e. g. Midwifery/HV specs to SLCN How do we get basic messages into communities Influencing schools as commissioners Developing analysis metrics Addressing so much unmet need | 20
Challenges to you • Upskilling the future workforce in their learning curriculum (MW, HVs, teaching staff , apprentices) • Raising level of skill required in EY settings. • Enabling inter agency data sharing • Developing a shared language we use same words with subtly different meanings • Do the Department works together? Conflicting agendas e. g. HV implementation plan increased provision ; transferred to LAs with no ring fencing. SLT: Highlighting unmet need but specialist services not sufficiently resourced to address thisd| 21
Thank You Any Questions? | 22