Dr MOHAMED NASR Lecturer Of Dermatology Venereology Zagazig
")


 n Protozoa: . Trichomonas vaginalis n Parasitic: • Pediculosis")

 is")
 n Urethral discharge often worse in morning, dysuria, urethral itching. GC")













 n n “Dermatitis-arthritis syndrome” u. Arthritis: 90% u. Characterized by")


 Endometritis Salpingitis, which")







 n Ceftriaxone 1 g IM or IV every 24 hours")


- Slides: 37
Dr. MOHAMED NASR Lecturer Of Dermatology & Venereology Zagazig University Sexually Transmitted Diseases (STDs)
Introduction n n Communicable disease transmitted mainly by sexual activity including genital-genital contact, anal-genital contact & oral-genital contact. May also be transmitted by blood & during birth.
Spectrum of STDs: n Bacterial: n Viral: • • Syphilis • • Gonorrhoea • • Non-gonococcal urethritis • • Chancroid • • Lymphogranuloma venereum • Donovanosis (Granuloma inguinale) HIV infection Genital wart Herpes genitalis Hepatitis B Cytomegalovirus
n Fungal: . Candidiasis (Moniliasis) n Protozoa: . Trichomonas vaginalis n Parasitic: • Pediculosis pubis • Scabies
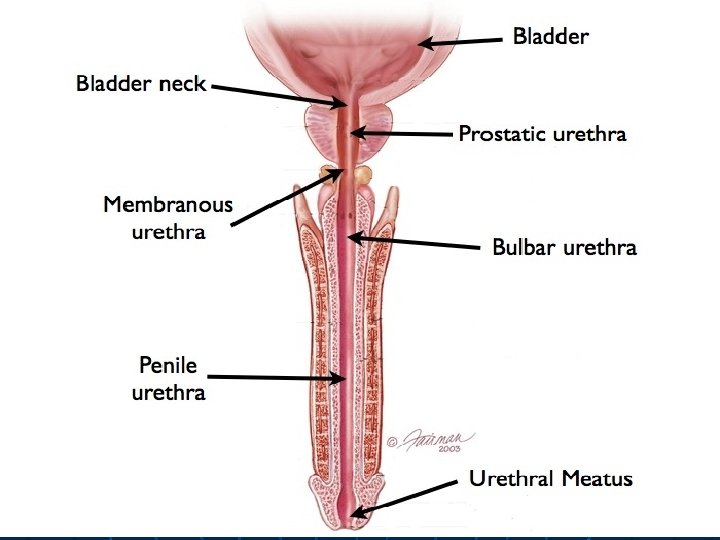
Urethritis Painful urethral discharge & testicular swelling are the most common presentations of symptomatic STDs in ♂.
Classification of urethritis 1. 2. Gonococcal urethritis. Non gonococcal urethritis. Non-gonococcal urethritis (NGCU) is > common than gonococcal urethritis.
Urethritis (Clinical Features) n Urethral discharge often worse in morning, dysuria, urethral itching. GC urethritis NGCU Organism(s) Gram (-)ve intracellular diplococci. Chlamydia trachomatis. Ureaplasma urealyticum. Trichomonas vaginalis. HSV: rare. Incubation period < 1 week 2 -3 weeks Discharge Amount Color +++ Yellowish-green (purulent) Often slight Gray, white, mucoid
Gonorrhoea n n n About 62 million cases of gonorrhoea are diagnosed each year worldwide. The causative organism, Neisseria gonorrhoeae, is a Gram negative diplococci. Infects non-cornified epithelium • Cervix • Urethra • Rectum • Pharynx • Conjunctiva
Transmission n n Gonorrhoea is always sexually transmitted in adults. Transmission is more efficient from males to females. The risk of acquisition from a single act of sexual intercourse with an infected partner is estimated at 30 - 70%. Vertical transmission also occurs. About 30% of babies born to infected mothers develop ophthalmia neonatorum, typically presenting in the first week after birth.
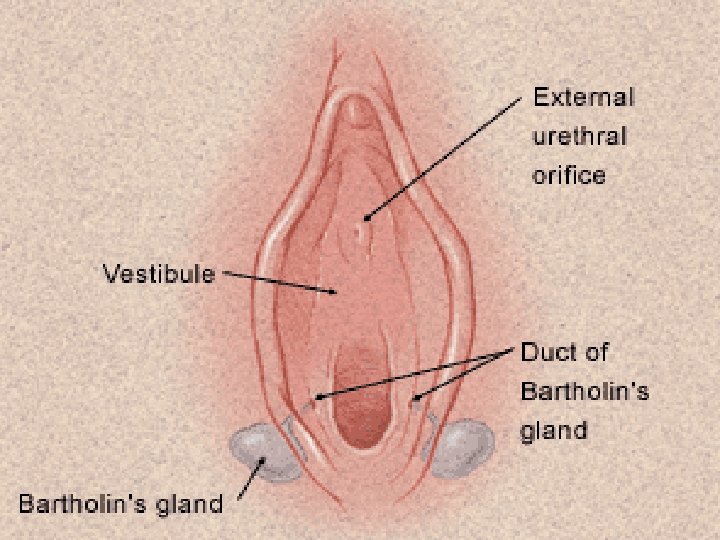
Gonococcal Infections in Women n n n n Cervicitis n Pharyngitis n DGI Urethritis Proctitis Accessory gland infection (Skene, Bartholin) Pelvic inflammatory disease (PID) Peri-hepatitis (Fitz-Hugh-Curtis) Pregnancy morbidity Conjunctivitis Many infections asymptomatic
Gonococcal Cervicitis Incubation 3 -7 days n. Symptoms: u. Vaginal discharge u. Dysuria u. Vaginal bleeding n. Cervical signs : u. Erythema u. Friability u. Purulent exudate n
Pelvic Inflammatory Disease Adhesions n n n Tube Symp. : bilateral lower abdominal pain. Signs: uterine/ adnexal tenderness, +/- fever. Laparoscopy may show hydrosalpinx, inflammation, abscess, adhesions. PID often silent
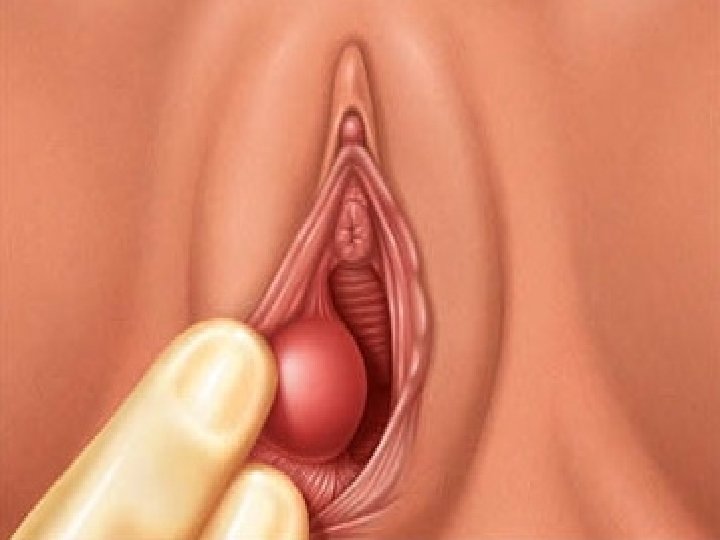
Bartholin’s Abscess n n Tender swelling in the lower 3 rd of the labia with difficulty in walking & sitting. Treatment: antibiotic, analgesic, drainage followed by marsupialization.
Gonococcal Infections in Men n n n n Pharyngitis Urethritis n DGI Epididymitis n Urethral stricture Proctitis n Penile edema Conjunctivitis Abscess of Cowper’s/Tyson’s glands Seminal vesiculitis Prostatitis Many infections asymptomatic
Gonococcal Urethritis n n n Incubation 2 -5 days. Abrupt onset of severe dysuria. Yellowish-green purulent urethral discharge.
Epididymitis § § Swollen painful epididymis usually unilateral. Epididymal tenderness or mass on exam.
Extra-genital gonococcal infection 1. Ano-rectal gonorhoea: * It results from rectal sex with an infected partner. * It is often asymptomatic but there may be a burning pain, tenesmus, pain on defaecation & bloody or mucopurulent stools.
2. Gonococcal pharyngitis * It always results from oro-genital coitus. * There is sore throat & pain on swallowing.
3. Gonorrhoea in children a. Ophthalmia neonatorum: * gonococcal eye infection of the newborn during passage through the birth canal. * it develops within 7 days of birth, always bilateral. * Lid edema, erythema and marked purulent discharge.
b. Gonococcal vulvo-vaginitis * before puberty, the vulval and vaginal epithelium is immature stratified squamous epithelium, this allows gonococcal infection to occur. * discharge on child’s underclothing. * vulva is red & oedematous.
4. Disseminated gonorrhoea (DGI) n n “Dermatitis-arthritis syndrome” u. Arthritis: 90% u. Characterized by fever, chills, skin lesions, arthralgia, tenosynovitis u. Less commonly, hepatitis, myocarditis, endocarditis, meningitis Rash characterized as macular or papular, pustular, hemorrhagic or necrotic, mostly on distal extremities.
Complications of gonorrhoea
Local complications in men n n n Para-urethral duct infection Tysonitis (infection of sebaceous glands) Periurethral abscess Epididymitis Penile oedema Prostatitis. Seminal vesiculitis.
Local complications in women n n Bartholinitis Skenitis (para-urethral gland infection) Endometritis Salpingitis, which may lead to peritonitis and tubo-ovarian abscesses Perihepatitis
Less commonly, disseminated infection occurs by haematogenous spread: n Septicaemia n Arthritis n Dermatitis n Endocarditis n Meningitis
GC Diagnostic Methods n n Gram stain smear Culture: - Enriched media e. g. Mcleod’s chocolate agar. - Selective media e. g. Thayer-Martin media. n n Antigen Detection Tests: EIA & DFA Nucleic Acid Detection Tests: • • • Probe Hybridization Nucleic Acid Amplification Tests (NAATs) Hybrid Capture
Gonorrhea Treatment Genital & Rectal Infections in Adults Recommended regimens: n n n Cefixime 400 mg PO x 1 or Ceftriaxone 125 mg IM x 1 or Ciprofloxicin 500 mg PO x 1 or Ofloxacin 400 mg PO x 1 or Levofloxacin 250 mg PO x 1 PLUS if chlamydia is not ruled out: n n Azithromycin 1 g PO x 1 or Doxycycline 100 mg PO BID x 7 d All sex partners within past 60 days need evaluation and treatment
Gonorrhea Treatment Genital & Rectal Infections in Adults Alternative regimens: § § § § Ceftizoxime 500 mg IM x 1 Cefotaxime 500 mg IM x 1 Cefoxitin 2 g IM x 1 plus probenecid 1 g PO x 1 Gatifloxacin 400 mg PO x 1 Lomefloxacin 400 mg PO x 1 Norfloxacin 800 mg PO x 1 Spectinomycin 2 g IM x 1
Gonorrhea Treatment Pregnancy Must avoid quinolones & tetracycline Recommended regimens: u Cefixime 400 mg PO x 1 u Ceftriaxone 125 mg IM x 1 PLUS if chlamydia is not ruled out: u u Azithromycin 1 g PO x 1 Other appropriate chlamydial regimen Test of cure in 3 -4 weeks
Gonorrhea Treatment Neonates Ophthalmia neonatorum prophylaxis: u. Silver nitrate 1% aqueous solution topical x 1 u. Erythromycin 0. 5% ointment topical x 1 u. Tetracycline 1% ointment topical x 1 Ophthalmia neonatorum treatment: u. Ceftriaxone 25 -50 mg/kg IV or IM x 1 NTE 125 mg NTE = not to exceed
Gonococcal conjunctivitis: u. Ceftriaxone 1 gm single IM once
Disseminated Gonococcal Infection (DGI) n Ceftriaxone 1 g IM or IV every 24 hours n Alternative Regimens Cefotaxime 1 g IV every 8 hours Ceftizoxime 1 g IV every 8 hours Ciprofloxacin 400 mg IV every 12 hours Ofloxacin 400 mg IV every 12 hours Levofloxacin 250 mg IV daily Spectinomycin 2 g IM every 12 hours n OR OR OR All of the preceding regimens should be continued for 24– 48 hours after improvement begins.
Gonorrhea Treatment Children Uncomplicated genital infection: • > 45 kg: same as adults • < 45 kg: ceftriaxone 125 mg IM x 1 (alternative spectinomycin 40 mg/kg IM x 1) Disseminated Gonococcal Infection: • Ceftriaxone 25 -50 mg/kg/d x 7 d • Treat for 10 -14 d if child weights > 45 kg