Dorothea Orems SelfCare Deficit Theory of Nursing 8440










. Dorothea Orem’s self care theory. Nursing Theories.")

- Slides: 16
Dorothea Orem’s Self-Care Deficit Theory of Nursing 8440 October 1, 2012 Jennifer Bauman, RN, BA, PCCN
Dorothea Orem: Background • • • Born: 1914 in Baltimore, Maryland Died: 2007 in Savannah, Georgia Diploma: Providence Hospital in Washington, DC BSN Ed. : 1939, Catholic University of America in Washington, DC MSN Ed. : 1945, Catholic University of America Honorary Doctorates: 1976 and 1980, Doctor of Science from Georgetown University and Incarnate Word College in San Antonio, Texas; 1988, Doctor of Humane Letters from Illinois Wesleyan University in Bloomington, Illinois Special Award: 1980, Catholic University of American Alumni Achievement Award for Nursing Theory Employment: staff nurse, private duty nurse, nurse educator, administrator, and consultant. Theory was first published in Nursing: Concepts of Practice in 1971, second in 1980, in 1995, and 2001
S-CDTN: Background • Orem served as nurse consultant with the Indiana State Board of Health from 1949 -1957 – Became “aware of the ability of nursing to do nursing, but their inability to talk about nursing” (Hartweg, p. 148). – Initial ideas about nursing in Indiana State Board of Health report • Further developed ideas as a consultant in the Office of Education, U. S. Department of Health, Education and Welfare – Task was to improve the nursing component of vocational nursing curriculum – Curriculum could not be determined until there was an understanding of the subject matter of nursing in general
S-CDTN: Questions • “What is nursing? ” • More specifically, “What is the domain and what are the boundaries of nursing as a field of practice and as a field of knowledge? ” • “What condition exists when judgments are made that people need nursing? ” – “The inabilities of people to care for themselves at times when they need assistance because of their state of personal health. ” (Hartweg, p. 148, as stated in 1959 by Orem)
S-CDTN: Theoretical Sources • “Her association with many nurses over the years provided many learning experiences, ” as well as work with graduate students and colleagues (Tomey and Alligood, p. 190) • Nursing theorist influences: Abdellah, Henderson, Johnson, King, Levin, Nightingale, Orlando, Peplau, Riehl, Rogers, Roy, Travelbee, Wiedenbach • Non-nursing theorist influences: Gordon Allport, Chester Barnard, Rene Dubos, Erich Fromm, Gartly Jaco, Robert Katz, Kurt Lewin, Ernest Nagel, Talcott Parsons, Hans Selye, Magda Arnold, William Wallace, Bernard Lonergan, and Ludwig von Bertalanffy
S-CDTN: Major Assumptions • People should be self-reliant and responsible for their own care and others in their family needing care. • People are distinct individuals. • Nursing is a form of action – interaction between two or more persons. • Successfully meeting universal and development selfcare requisites is an important component of primary care prevention and ill health. • A person’s knowledge of potential health problems is necessary for promoting self-care behaviors. • Self care and dependent care behaviors learned within a social and cultural context.
S-CDTN: Major Assumptions • Human beings require continuous, deliberate inputs to themselves and their environments to remain alive and function in accordance with natural human endowments. • Human agency, the power to act deliberately, is exercised in the form of care for self and others in identifying needs and making needed inputs. • Mature human beings experience privations in the form of limitations for action in care for self and others involving and making of life-sustaining and function-regulating inputs. • Human agency is exercised in discovering, developing, and transmitting ways and means to identify needs and make inputs to self and others. • Groups of human beings with structured relationships cluster tasks and allocate responsibilities for providing care to group members who experience privations for making required, deliberate input to self and others.
S-CDTN: Interrelated Theories • Theory of Self-Care Deficit – Question: “When and why do people require the health service nursing? ” – Central Idea: Why people can be helped through nursing (T&A). Individuals experience limitations that do not allow them to meet their self-care needs. Limitations may be a health condition, internal (e. g. age), or external (e. g. unexpected death in family). • Theory of Self-Care – Question: “What is self-care and what is dependent care? ” – Central Ideas: Why and how people care for themselves (T&A). Self-care as a learned behavior and therefore varies by the cultural and social context of the individual. Self-care as deliberate action (i. e. “performed with purpose”). – Dependent care by a responsible adult replaces self-care if self-care abilities are not yet mature (e. g. infant) or are inoperable (e. g. coma). • Theory of Nursing Systems – Questions: “What do nurses do when they nurse? ”, “What is the product made by nurses? ”, and “What results are sought by nurses? ” – Central Idea: Relationships that must be brought about and maintained for nursing to be produced (T&A). Nurses determine if nursing help is needed, design a plan of care, and implement. “The goal of the nursing system is to increase the patient’s capabilities to meet a needs, or requisite, or to decrease the demand” (Hartweg, p. 157).
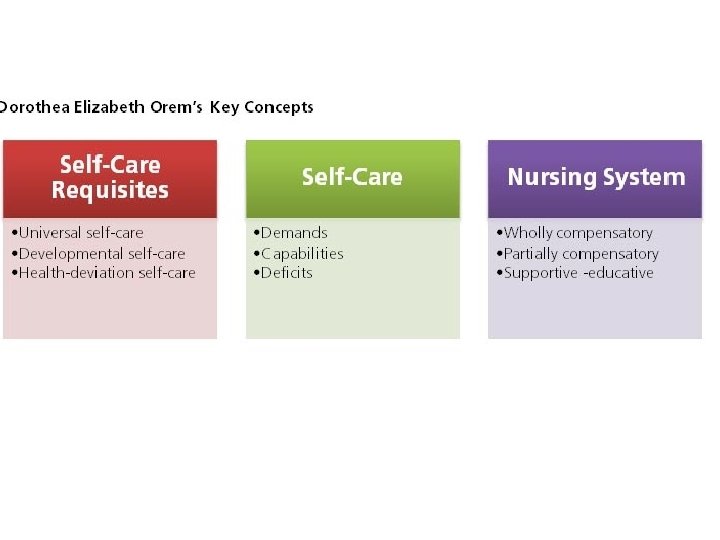
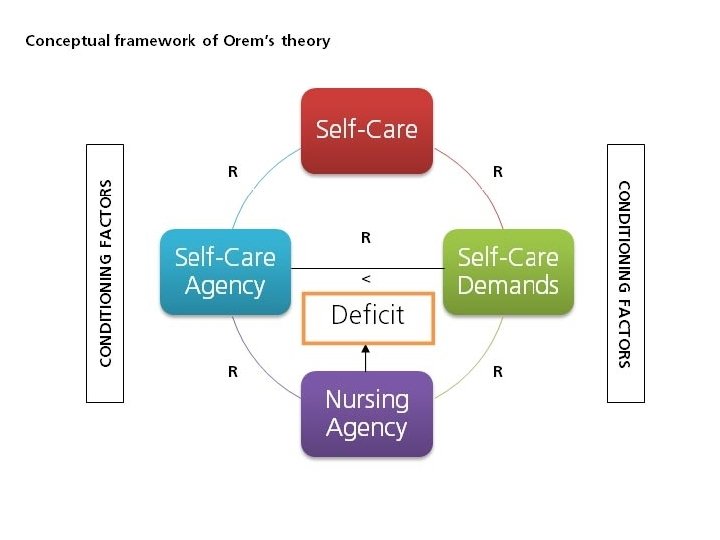
• Self-care S-CDTN: Concepts – “The practice of activities that individuals initiate and perform on their own behalf in maintaining life, health, and well-being” (Hartweg, p. 158). • Self-care agency – “The power of individuals to engage in self-care and the capability for self-care” (Hartweg, p. 161). • Therapeutic self-care demand (TSCD) – “The ‘summation of measures of self-care required at moments in time and for some duration’” (Hartweg, p. 164, as stated by Orem, 1991). Also includes the selfcare requisite, or generalized purpose for which individual performs self-care. • Self-care deficit – Describes the relationship between self-care, self-care agency, and TSCD. Can be greater than, equal to, or less than/not adequate. Self-care deficit must exist currently or in future for nursing need to be legitimate. • Nursing agency – “The ‘complex property or attribute of persons educated and trained as nurses that is enabling when exercised for knowing and helping others know their therapeutic self-care demands, for helping others meet or in meeting their therapeutic self-care demands, and I helping others regulate the exercise or development of their selfcare agency or their dependent-care agency’” (Hartweg, p. 168, as stated by Orem, 1991). • Nursing system – “’All the actions and interactions of nurses and patients in nursing practice situations’” (Hartweg, p. 169, as stated by Orem, 1985).
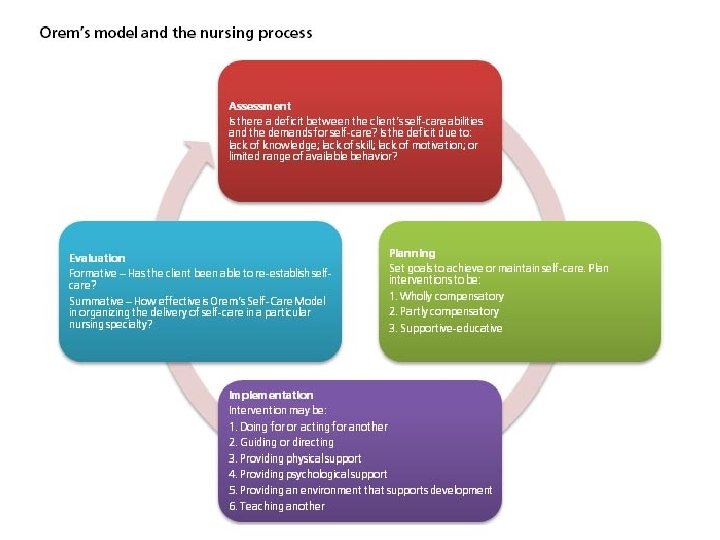
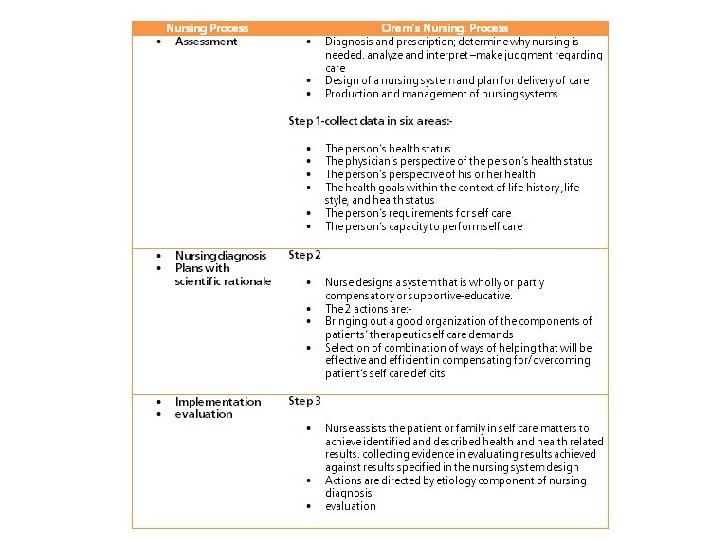
Implications for Practice and Research • Implications for Practice – Universality of theory – Application to ADPIE Nursing Process • Possible Research Topics – Instruments for measuring the conceptual elements (self-care, self-care deficit) – Use in specific populations (diabetes, hemodialysis, obesity)
References • Current Nursing (4 Feb 2012). Dorothea Orem’s self care theory. Nursing Theories. Retrieved September 19, 2012, from http: //currentnursing. com/nursing_theory/self_care_deficit_theor y. html. • De Lara, R. (17 July 2010). Dorothea Elizabeth Orem’s theory of self care. Retrieved October 1, 1012, from http: //upoun 207 tfn. blogspot. com/2010/07/dorothea-oremstheory-of-self-care_17. html. • Hartweg, D. L. (1995). Dorothea Orem: Self-care deficit theory. In C. M. Mc. Quiston and A. A. Webb (Eds. ), Foundations of nursing theory: Contributions of 12 key theorists (pp. 139 -202). Thousand Oaks, CA: Sage Publications, Inc. • Taylor, S. G. (2002). Dorothea E. Orem: Self-care deficit theory of nursing. In A. M. Tomey and M. R. Alligood (Eds. ), Nursing theorists and their work (5 th Ed. , pp. 189 -211). St. Louis, Missouri: Mosby, Inc.
Philosophical Considerations • Moderate realism, as described by Wallace – Good description of moderate realism: http: //books. google. com/books? id=m 9 b. Lp 0 o. F 9 BIC&pg=PT 338&lpg=P T 338&dq=moderate+realism+wallace&source=bl&ots=4 R 1 U 0 OVd. Hx& sig=Xdj. ZEV 3 w 1 Qegkva. XX 3_f. C 13 l 6 WU&hl=en&sa=X&ei=5 ENm. ULi. XIPkyw. HWr. YCg. DQ&ved=0 CC 4 Q 6 AEw. Aw#v=onepage&q=moderate%20 r ealism%20 wallace&f=false • According to Banfield, “‘the view of human beings as dynamic, unitary beings who exist in their environments, who are in the process of becoming, and who posses free-will as well as other essential human qualities’