CPPD DEPOSITION DISEASE z Calcium Pyrophosphate Dihydrate Epidemiology









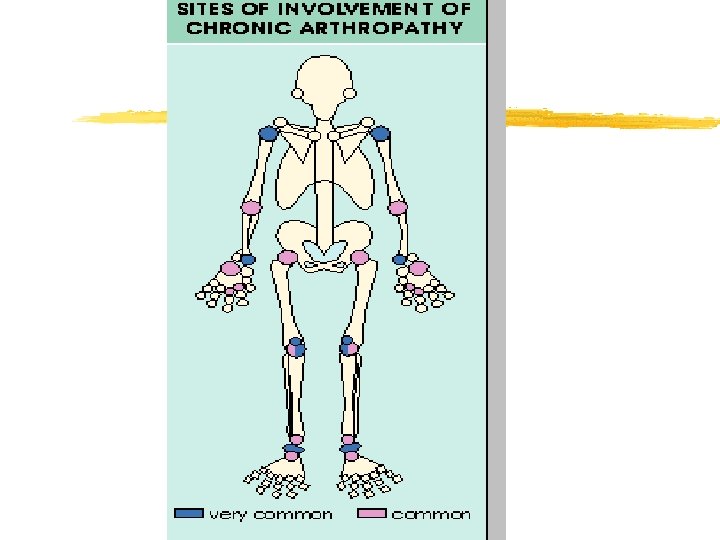
 z May be precipitated by trauma z Knee, wrist, shoulder, ankle, elbow,")














- Slides: 34
CPPD DEPOSITION DISEASE z. Calcium Pyrophosphate Dihydrate
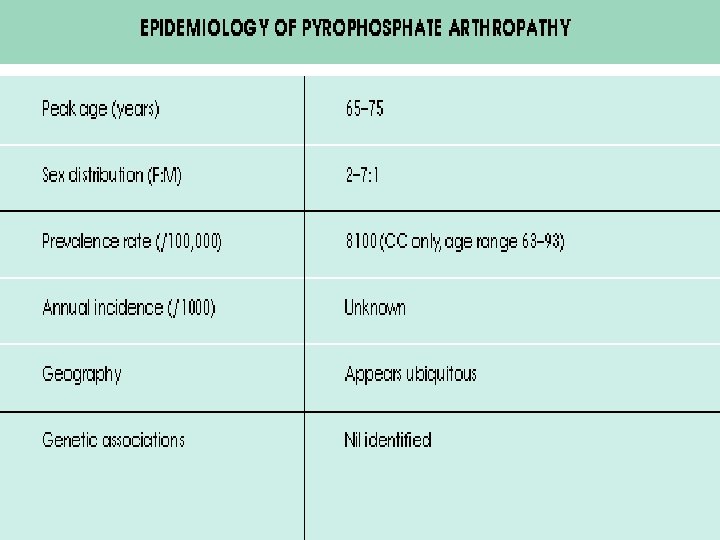
Epidemiology z. Most common in the elderly z 10 to 15% of persons 65 to 75 years old and 30 to 60% of those more than 85 years old z. In most cases this process is asymptomatic
What is CPPD Ca 2 P 2 O 2. 2 H 2 O
Etiology z Cause of CPPD deposition is uncertain z Because over 80% of patients are more than 60 years old and 70% have preexisting joint damage from other conditions, it is likely that biochemical changes in aging cartilage favor crystal nucleation z There is an increased production of inorganic pyrophosphate and decreased levels of pyrophosphatases in cartilage extracts from patients
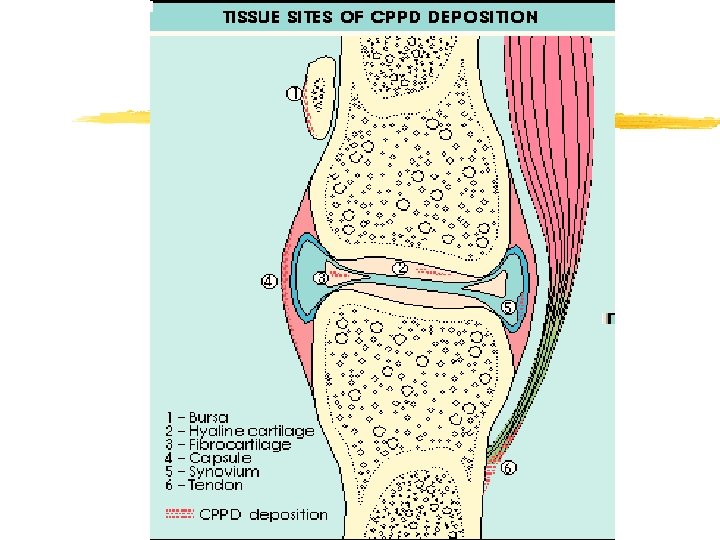
Pathophysioloy z. The release of CPPD crystals into the joint space is followed by the phagocytosis of these crystals by neutrophils, which respond by releasing inflammatory substances. In addition, neutrophils release a glycopeptide that is chemotactic for other neutrophils, thus augmenting the inflammatory events
Pathophysioloy z. A minority of patients with CPPD arthropathy have metabolic abnormalities or hereditary CPPD disease
Conditions associated with CPPD z. Aging z. Hyperparathyroidism z Hemochromatosis z Hypophosphatasia z. Hypomagnesemia z. Chronic thophaceous gout z. Hereditary
Clinical Manifestations z. CPPD arthropathy may be asymptomatic, acute, subacute, or chronic or cause acute synovitis superimposed on chronically involved joints
Clinical Manifestations z. Pseudogout z. Pseudo-osteoarthritis z. Pseudo-Rheumatoid z. Destructive arthropathy z. Bursitis, tendinitis, enthesitis
Acute Arthritis(Pseudogout) z May be precipitated by trauma z Knee, wrist, shoulder, ankle, elbow, and hands z Symptoms are the same as any acute arthritis z Occasionally systemic symptoms: Fever z Self limited z Patients are asymptomatic between attacks
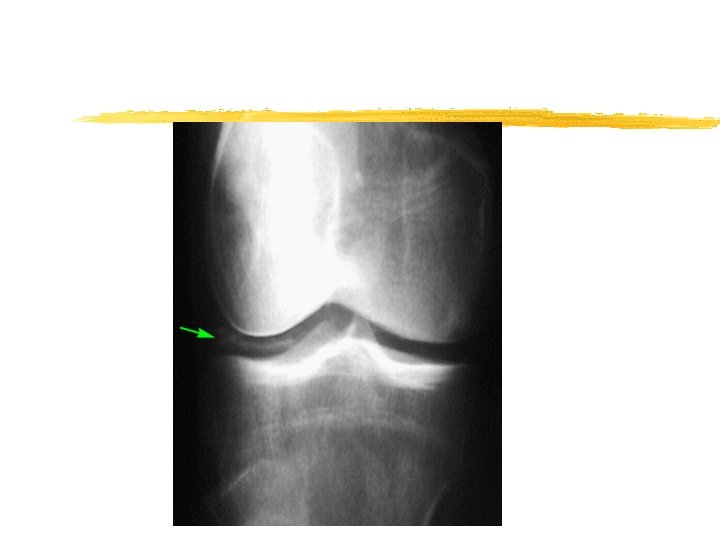
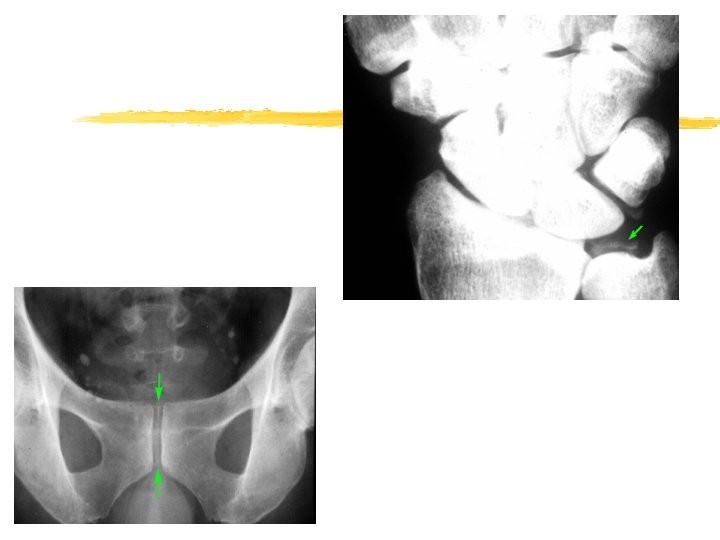
Imaging z Chondrocalcinosis
IS all chondrocaclnosis caused by CPPD z. No z. Other calcium salts such as calcium hydroxyapatite z. Ochronosis
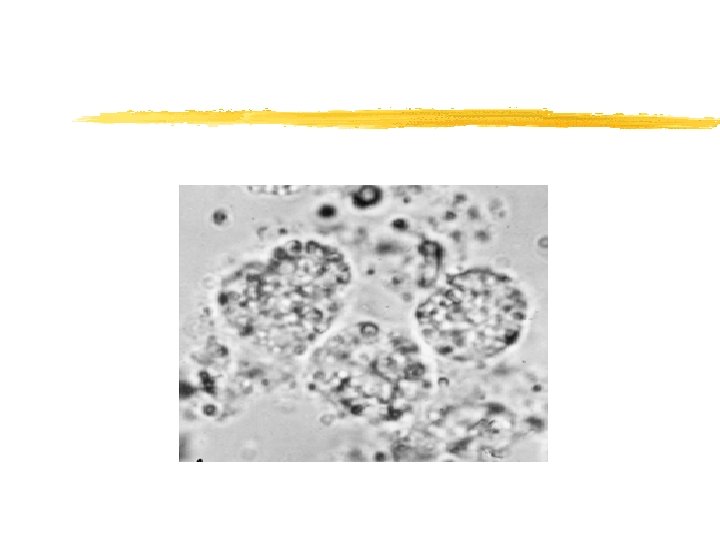
Synovial fluid z. Several thousand cells to 100, 000 cells/u. L z. Mean being about 24, 000 cells/u. L z. Predominant cell being the PMN
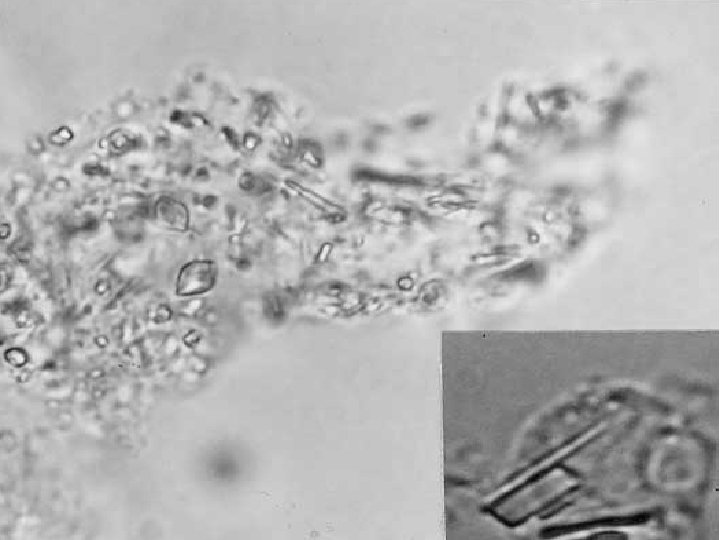
Diagnosis z Polarization microscopy usually reveals rod - shape or rhomboid crystals inside fibrin and in PMN
Pseudo-osteoarthritis z Pattern of joint involvement z Knee, MCP, wrist, elbow , shoulder z More likely to be symmetrical z Chondrocalcinosis
Pseudo-Rheumatoid z. RF 10% z. Involvement of hands z. CPPD Crystals z. X-ray
Treatment z. NSAIDS z. Colchicin z. Corticosteroids
CALCIUM HYDROXYAPATITE DEPOSITION DISEASE
Pathogenesis z HA is the primary mineral of bone z HA may be released from exposed bone and cause the acute synovitis z Most patients with HA arthropathy are elderly. z Periarticular and articular deposits may coexist and be associated with acute and/or chronic damage to the joint capsule, tendons, bursa, or articular surfaces.
Clinical z. The most common sites of HA deposition include bursa and tendons in and/or around the knees, shoulders, hips, and fingers z. Clinical manifestations include: asymptomatic radiographic abnormalities, acute synovitis, bursitis, tendinitis, and chronic destructive arthropathy
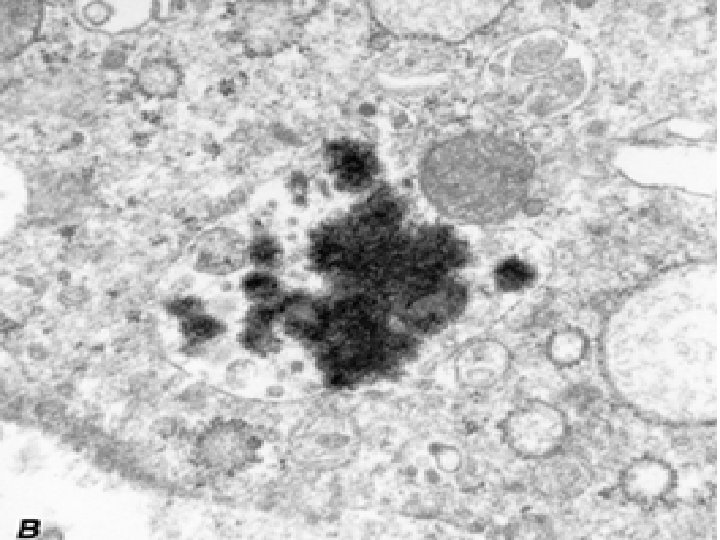
Diagnosis z. Intra- and/or periarticular calcifications zcrystals are very small, and can only be seen by electron microscopy.