Atropine use in vasovagal response Dr Naila Rafique







 Check vital signs Lay")






- Slides: 15
Atropine use in vasovagal response ` Dr Naila Rafique Clinical governance day 24/05/2017
Introduction Any invasive procedure in a non-anaesthetised woman including IUC fitting can trigger a vasovagal response Significant slowing of the HR(bradycardia-<60/min) & drop in BP Inadequate oxygenation & blood flow to brain with loss of consciousness Assoc. with transient period of twitching or brief seizure
Most patients do not get sx unless HR <40/min An appropriately trained asst. should be present during cx instrumentation procedures May be reqd. to call for further asst. , monitor the pt’s condition or perform BLS True incidence of SH related adverse events unknown
FSRH Service Standards for Resuscitation 2016 Basic resuscitation equipment should be available in all clinics Recommended emergency equipment Ø Selection of needles and syringes Ø Pocket mask Ø O 2 face mask Ø Airways Ø Adjustable couch Ø Pulse oximeter desirable
‘Drugs required for resuscitation must be available, accessible, clearly labelled, adequately maintained and their location know to all staff. ’ Recommended emergency drugs Ø Adrenaline 0. 5 mg IM(0. 5 ml of 1: 1000 inj. ) Ø Atropine 500 or 600 mcgms IV/IM (2 doses) Ø Oxygen -must be available for planned intra-uterine instrumentation(desirable for more minor procedures)
Symptoms & Signs C/o faintness/feeling light headed and dizziness Slow pulse rate/bradycardia Low BP Pallor and sweating Nausea and vomiting Loss of consciousness
Treatment Use ABCDE approach Airway, Breathing, Circulation, Disability, Exposure Stop Call for help Assess patient
C-Circulation Look for signs of shock(pallor, sweating, feeling faint, nausea) Check vital signs Lay the patient flat ASAP and raise legs to improve VR Vast majority of vasovagal attacks will improve with these measures Observe the patient – keep them laying down till feeling better
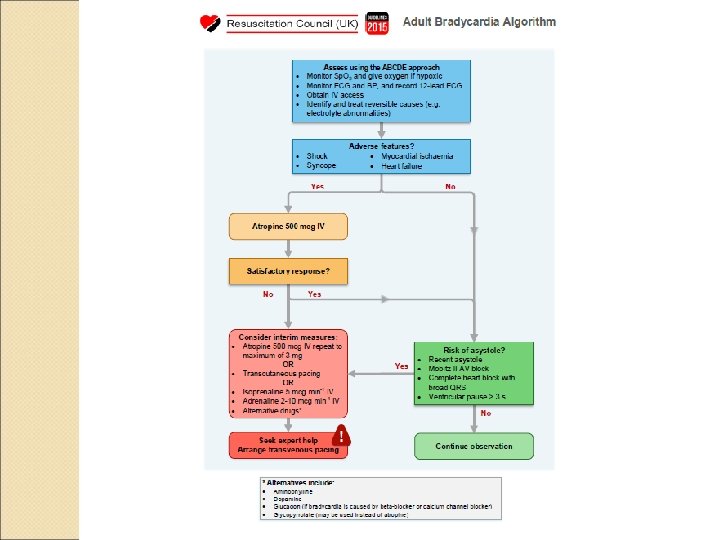
the pt fails to improve and pulse remains slow, use of atropine is warranted Whenever possible RC(UK)bradycardia algorithm should be foll. Single dose of Atropine 500 -600 mcg IV foll. by saline flush HR will usually increase within few minutes If no improvement summon emergency assistance and repeat Atropine If
• If staff unable to gain IV access give IM Atropine (500 -600 mcg) Not part of RC bradycardia algorithm Recommended in BNF Given mid thigh with long needle Increase in HR significantly slower than IV dose If pt’s condition deteriorates/no improvement within 10 minutes, repeat atropine while awaiting emergency services
Ambulance responders will decide further mx The Human Medicines Act 2012 permits nurses to give certain drugs without prescription for the purpose of saving life in an emergency (http: //www. legislation. gov. uk/uksi/2012/1916/conte nts/made)
• If pt becomes unresponsive i. iii. • i. ii. check for signs of life(breathing, circulation) start CPR if no signs call 999 If signs of life present(pt breathing normally but unconscious) Ensure full recovery position Call 999
12 lead ECG not immediately necessary to diagnose and treat a clinically symptomatic bradycardia RC(UK) ALS advice is to record a 12 lead ECG at the earliest available opportunity If the paramedical services are summoned they will always record an ECG
Thank you