Allocation systems in liver transplantation Farzad Kakaei MD





 • Principles of organ allocation should be based on objective criteria")
 • Initially developed for survival prediction after TIPS. •")
) + (0.")
 HCC HEPATOPULMONARY SYNDROME")




- Slides: 16
Allocation systems in liver transplantation Farzad Kakaei, MD, Associate professor of surgery, Tabriz University of medical sciences, Tabriz, Iran
Introduction • Approaches to the problem of graft scarcity, • Increasing donor pool (living, brain death, cardiac death) • Improving alternative treatments for liver diseases and hepatocellular cancer. • Liver allocation policies • The goal of allocation systems : the best possible outcomes for the waiting list • We need for change in our policy because of : • Changes in the etiology of cirrhosis over time • Recent expansion of indications for liver transplantation (including cholangiocarcinoma and colorectal liver metastases) • Geopolitical and social environments • Expansion of liver transplant centers
A brief history • Procurement and allocation of donor organs was performed locally by individual hospital-based teams in the early era of liver transplantation • Reducing the mortality rate to less than 10% by 1984 results in a series of high profile controversial transplants with accusations of bias, arbitrary decision-making and manipulation of transplant waiting lists in return for financial donations • National Organ Transplant Act in 1984 (criminalizing financial compensation for donor organs). • Regional networks for organ procurement and distribution were established with the aim of transferring the responsibility for organ allocation from individual physicians to evidence-based, objective and transparent algorithms based primarily on clinical need • Similar fundamental principles were subsequently adopted by all countries and centres.
Principles of organ allocation
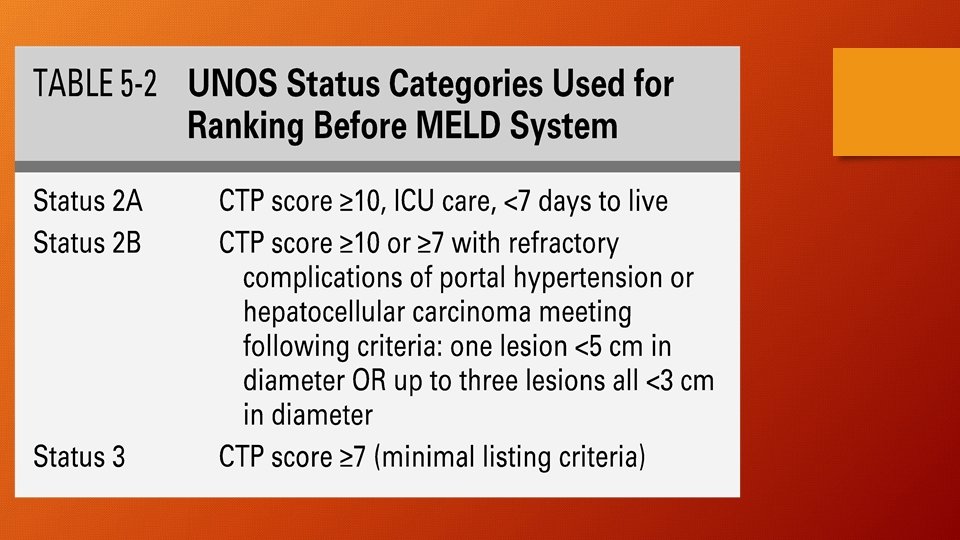
Evolution of liver allocation • Before 1997 : Center based, based on surrogate markers of clinical need, such as waiting time and patient location (intensive care, hospitalized, ambulatory). • candidates could be listed earlier than necessary • simply be hospitalized to obtain more points. • 1997: UNOS satus Category based on Child-Turcotte- Pugh (CTP) {ascites, encephalopathy, BR, Alb, PT} have several limitations: • Assessments of encephalopathy and ascites are considerably subjective. • It fails to consider renal function as a prognostic variable, • It does not discriminate between patients who have high bilirubin or low albumin below 28 g/dl
Final Rule (1999) • Principles of organ allocation should be based on objective criteria of medical urgency, rather than waiting time • “more accessible, equitable and efficient allocation of organs” • “minimal suitability criteria for transplant candidates” • “distribution of organs over as broad a geographical range as possible.
The MELD era (February 2002) • Initially developed for survival prediction after TIPS. • Based on bilirubin, creatinine and INR • Introduced to the US in 2002 and used by many countries since. • Reduction in waiting list mortality • small overall increase in early post-transplant mortality • Failure to account for elevations in INR and creatinine for reasons other than liver disease or inaccurate laboratory results • Failure to include other problems such as pruritus, ascites, GIB, HCC, polycystic liver disease, Caroli syndrome, bile duct injury, liver trauma and acute liver failure. • Systematically biased against women • No space for donor-recipient matching
MELD-Na or UKELD • UKELD = 5 x ((1. 5 x Ln(INR)) + (0. 3 x Ln(creatinine μmol/L)) + (0. 6 x Ln(bilirubin μmol/L)) – (13 x LN(Na+)) + 70) • MELD = 3. 8 x Ln(bilirubin mg/d. L) + 11. 2 x Ln(INR) + 9. 6 Ln(creatinine mg/d. L) • Listing by MELD>=18 or UKELD >=49 • Within any DONOR SERVICE AREA, • First allocated by the highest MELD • If two or more candidates have the same score, the liver is allocated to the candidate with the most waiting time. • MELD allocation does not apply to status 1 A or 1 B candidates
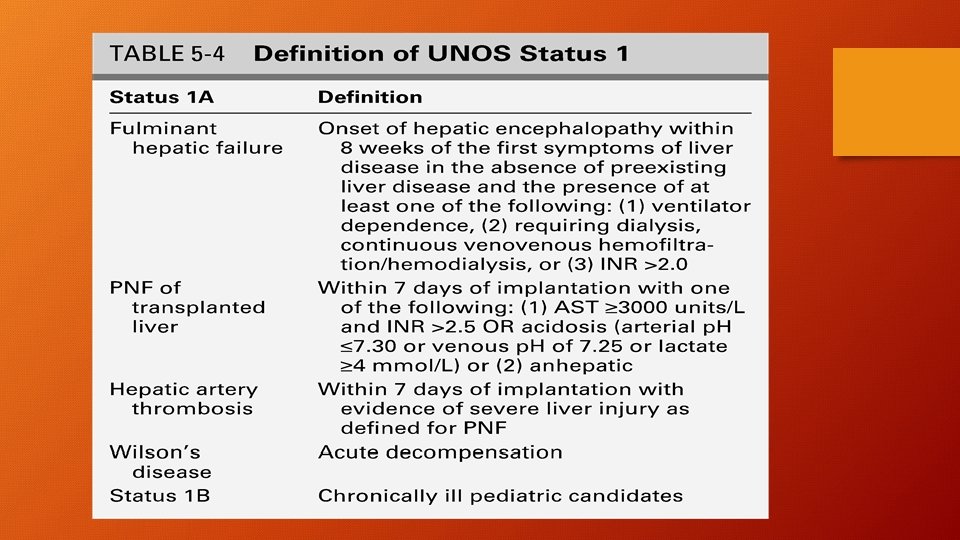
MELD exceptions • • • UNOS STATUS 1 (acute hepatic failure) HCC HEPATOPULMONARY SYNDROME (Pa. O 2<60 with a confirmed shunt) PORTOPULMONARY SYNDROME (25<PAP<35 mm. Hg) CYSTIC FIBROSIS FAMILIAL AMYLOID SYNDROME PRIMARY HYPEROXALURIA HILAR CHOLANGIOCARCINOMA FAMILIAL HYPERCHOLESTROLEMIA, Polycystic liver disease, … (? )
UK status prior to 2018 • Allocation on a regional basis • Priority given to the transplant center assigned to a designated organ recovery zone. • Individual waiting list • Compatibility (size and blood group) • UKELD • Logistical benefits • Minimizing graft cold ischemic time, • Perpetuate some ongoing geographical inequity in organ allocation.
UK status after 2018 Transplant Benefit Score • https: //transplantbenefit. org/
European calculators • https: //www. efclif. com/scientific-activity/score-calculators/clif-c -aclf • https: //www. efclif. com/scientific-activity/score-calculators/clif-c -ad
What is the future of liver allocation? • A different way of modelling (artificial intelligence) • Consider the use of expanded criteria grafts (DCD, Normothermic regional perfusion and ex-situ liver perfusion) • Allow for expansion of recipient selection criteria (colorectal metastasis, HCC beyond Milan criteria, cholangiocarcinoma) • Interaction with living donor transplantation • Going beyond traditional outcomes – quality of life measures