Radiological Category Thoracic Chest Principal Modality 1 CT
: CT Principal Modality (2): none Case Report")





 in")


 Tree-in-bud: Currently unknown. Negative for AFB, PCP, or fungal infection. Respiratory cultures")
- Slides: 11
Radiological Category: Thoracic Chest Principal Modality (1): CT Principal Modality (2): none Case Report #0031 Submitted by: Corinne Deurdulian , M. D. Faculty reviewer: Sandra A. A. Oldham, M. D Date accepted: 28 October 2003
Case History 22 y. o. female with history of schizophrenia, recently intubated for 1 week for drug overdose. Patient developed chronic cough, great difficulty breathing and wheezing after extubation.
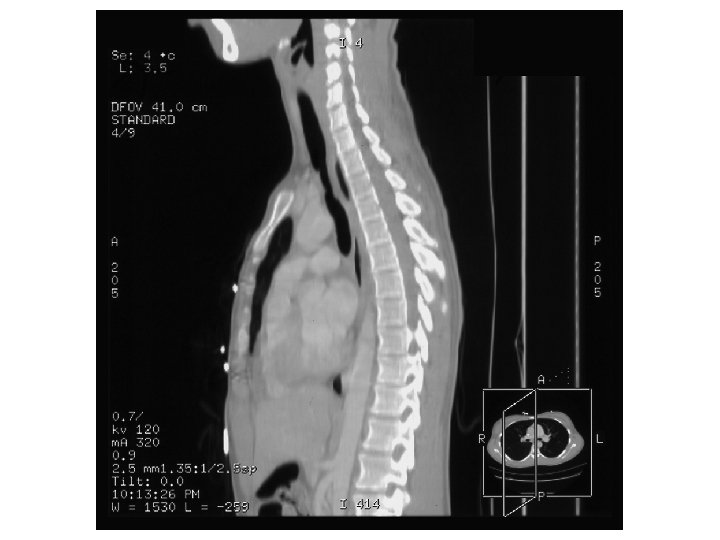
Radiological Presentations
Radiological Presentations
Radiological Presentations
Test Your Diagnosis Which one of the following is your choice for the appropriate diagnosis? After your selection, go to next page. PARENCHYMAL PROCESS • RSV pneumonia • Mycoplasma pneumonia • Mycobacterial infection • Metastatic disease • Aspiration TRACHEA • Sarcoid • Tracheal tumor • Trauma/ Iatrogenic • Infection (TB, fungal)
Findings and Differentials Pulmonary Parenchymal Findings: Nodules and branching linear opacities (aka “tree-in-bud”) in both lower lobes Differentials for tree-in-bud: • Infection: Mycobacterial, bronchopneumonia, viral, fungal, aspiration • Bronchial disease: Bronchitis/ bronchiolitis, diffuse panbronchiolitis • Congenital: Cystic Fibrosis, Dyskinetic Cilia Syndrome • Immunologic: ABPA • Lymphatic disease: Lymphangitis carcinomatosa, sarcoid, Langerhans Histiocytosis • Mets: Hematogenous mets (very rare)
Findings and Differentials Tracheal Findings: Focal tracheal narrowing Differentials for tracheal narrowing: • Traumatic injury/ iatrogenic (e. g. endotracheal intubation) • Congenital tracheal stenosis • Infection: fungal, TB • Inflammatory: sarcoidosis, amyloidosis, relapsing polychondritis • Neoplasm: squamous cell carcinoma, chondroma, fibroma, papilloma
Discussion In both lower lobes, there are multiple small nodules and branching linear opacities in a centrilobular distribution, also described as a “tree-in-bud” pattern. This pattern represents bronchiolar dilatation and filling by mucus, pus, or fluid, resembling a branching tree with buds at the tips of the branches. This finding is indicative of airway disease, and is particularly common in endobronchial spread of infection with mycobacteria (such as TB) and viruses (such as RSV and adenovirus). Other causes include cystic fibrosis, diffuse panbronchiolitis, and chronic airway infection due to asthma, chronic bronchitis, and bronchiectasis. Focal tracheal stenosis may be caused by a number of conditions, the most common of which is intubation-related injury. Overinflation of the cuff can produce blood flow obstruction, leading to inflammation and erosion of the tracheal mucosa and later, necrosis and destruction. Cuff strictures can occur as little as 36 hours after intubation and usually become symptomatic an average of 5 weeks later. The other causes of narrowing (congenital, infectious, inflammatory, and neoplastic) are much less common. Prior to the patient’s illness, she had no history of tracheal anomaly. The patient developed stridor after prolonged intubation, which would make intubation the most plausible etiology for the imaging findings. References: AJR 1998; Collins J, et al. CT patterns of bronchiolar disease: What is “Tree-in-Bud”? 171: 365370 Mc. Loud T. Thoracic Radiology: The Requisites 1998 Baylor College of Medicine Dept. of Otorhinolaryngology Grand Rounds Archives 1991; Eicher S. Benign Tracheal Stenosis Chest Surg Clin N Am. 2003; Wain J. Postintubation tracheal stenosis. 13(2): 231 -46
Diagnosis 1) Tree-in-bud: Currently unknown. Negative for AFB, PCP, or fungal infection. Respiratory cultures have been negative, but the patient was incompletely treated with antibotics. Aspiration is therefore most likely. 2) Tracheal stenosis: Iatrogenic related to recent intubation. She has been treated with bronchoscopically guided tracheal dilatation x 2. Due to her young age, her physicians are opting for dilatation of the trachea rather than stent placements.